

Comparative United States autoimmune disease rates for 2010-2016 by sex, geographic region, and race
- PMID: 31733367
- PMCID: PMC6925958
- DOI: 10.1016/j.autrev.2019.102423
Comparative United States autoimmune disease rates for 2010-2016 by sex, geographic region, and race
Abstract
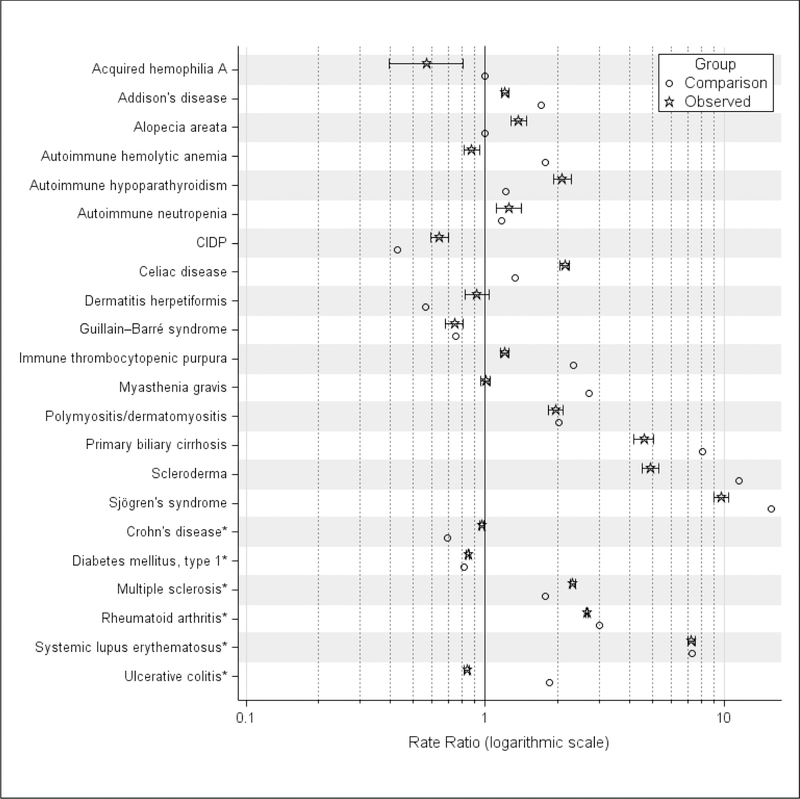
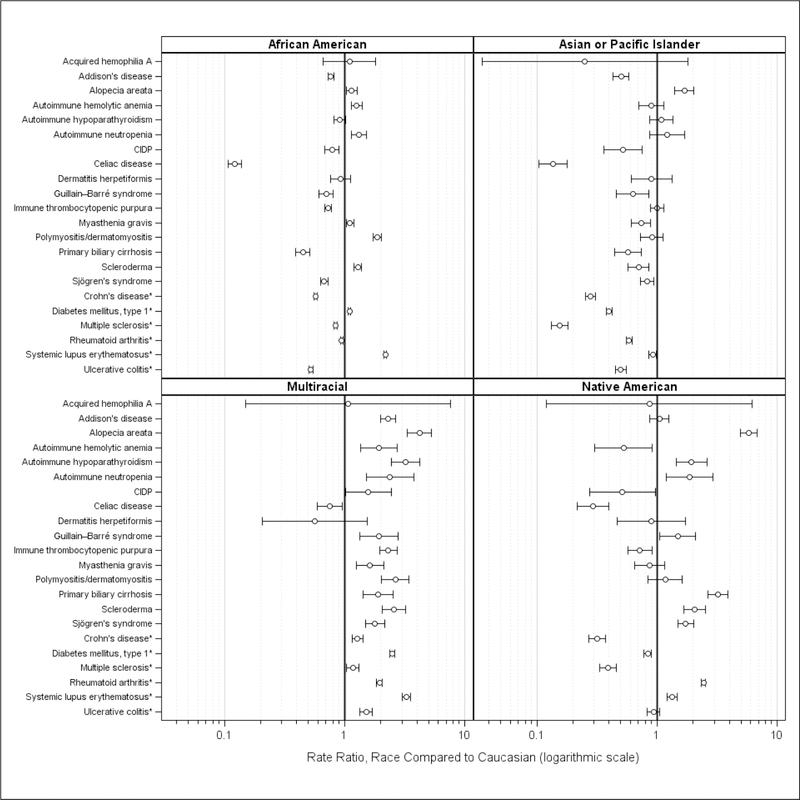
Purpose: AIDs may disproportionately impact specific racial groups, but autoimmune (AID) prevalence information by minority racial group is sparse for many AIDs. The objective of this analysis was to supplement previously published AID prevalence rates by providing information on race rate ratios (minority race populations compared to Caucasian populations) in the United States. Preliminary to estimating race rate ratios, contemporary US-specific, health care utilization-based AID prevalence rates and female-to-male ratios were estimated and compared to previously published AID prevalence rates.
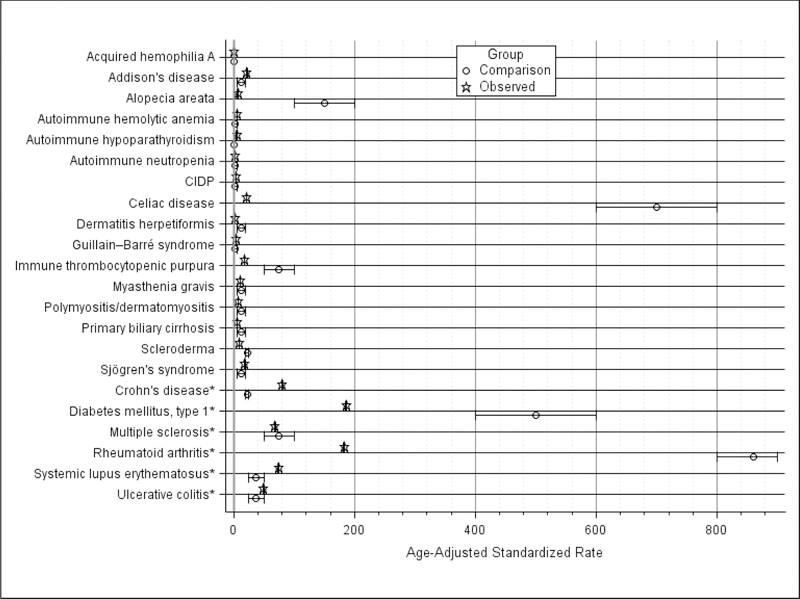
Methods: We used a large national electronic medical record database of 52 million individuals to estimate age-adjusted direct standardized rates for 22 AIDs for 2010 through 2016 by gender, race, and US census division. These were compared to previously published estimates.
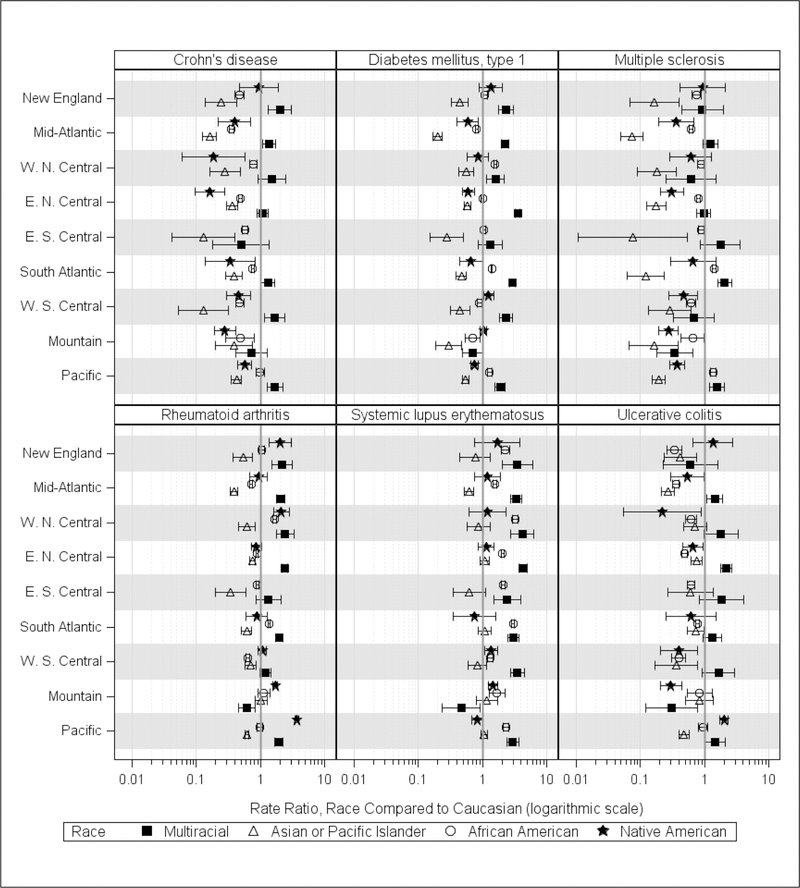
Results: Female-to-male ratios were comparable with published studies. Almost all observed Multiracial AID rates were significantly higher than Caucasian rates, as well as 9 of 22 AID rates observed among Native Americans and 8 of 22 AID rates estimated among African-American patients. Regional variation was noted: highest African-American systemic lupus erythematosus rates were observed in the West North Central and South Atlantic divisions, highest African-American multiple sclerosis rates in the South Atlantic and Pacific divisions, and highest Native American rheumatoid arthritis rates in the West North Central, Mountain, and Pacific divisions.
Conclusions: Substantial AID heterogeneity exists by race and by geographic area. An important research area is further exploring factors related to heterogeneity such as potential interactions between genetic susceptibility and environmental factors.
Keywords: Autoimmune disease; Minority groups; North American; Prevalence.
Copyright © 2019 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- U.S. National Institutes of Health (NIH). Biennial Report of the Director. National Institutes of Health: Fiscal Years 2014 & 2015. https://report.nih.gov/biennialreport/ [accessed 17 January, 2019].
-
- Hayter SM, Cook MC. Updated assessment of the prevalence, spectrum and case definition of autoimmune disease. Autoimmun Rev. 2012;11:754–65. - PubMed
-
- Damoiseaux JGMC, Cohen Tervaert JW. The definition of autoimmune disease: are Koch’s postulates applicable? Netherlands J Med. 2002;60:266–8. - PubMed
-
- National Institutes of Health (NIH) Autoimmune Diseases Coordinating Committee. Progress in autoimmune diseases research. (Publication No. 05–5140). March 2005. https://www.niaid.nih.gov/sites/default/files/adccfinal.pdf [accessed 17 January, 2019].
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
