

School-based interventions to prevent anxiety and depression in children and young people: a systematic review and network meta-analysis
- PMID: 31734106
- PMCID: PMC7029281
- DOI: 10.1016/S2215-0366(19)30403-1
School-based interventions to prevent anxiety and depression in children and young people: a systematic review and network meta-analysis
Erratum in
-
Correction to Lancet Psychiatry 2019; 6: 1011-20.Lancet Psychiatry. 2020 Sep;7(9):e59. doi: 10.1016/S2215-0366(20)30352-7. Lancet Psychiatry. 2020. PMID: 32828170 Free PMC article. No abstract available.
Abstract
Background: Rates of anxiety and depression are increasing among children and young people. Recent policies have focused on primary prevention of mental disorders in children and young people, with schools at the forefront of implementation. There is limited information for the comparative effectiveness of the multiple interventions available.
Methods: We did a systematic review and network meta-analysis, searching MEDLINE, Embase, PsycINFO, and Cochrane Central Register of Controlled trials for published and unpublished, passive and active-controlled randomised and quasi-randomised trials. We included educational setting-based, universal, or targeted interventions in which the primary aim was the prevention of anxiety and depression in children and young people aged 4-18 years. Primary outcomes were post-intervention self-report anxiety and depression, wellbeing, suicidal ideation, or self-harm. We assessed risk of bias following the Cochrane Handbook for Systematic Reviews of Interventions. We estimated standardised mean differences (SMD) using random effects network meta-analysis in a Bayesian framework. The study is registered with PROPSERO, number CRD42016048184.
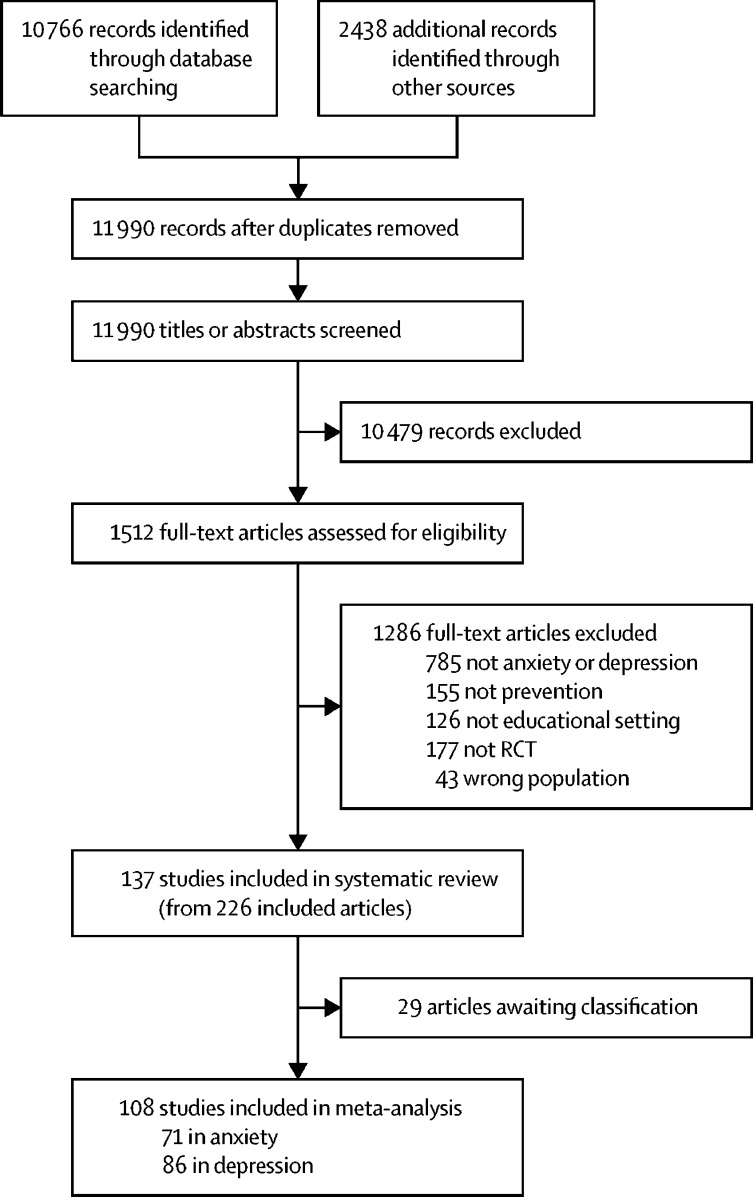
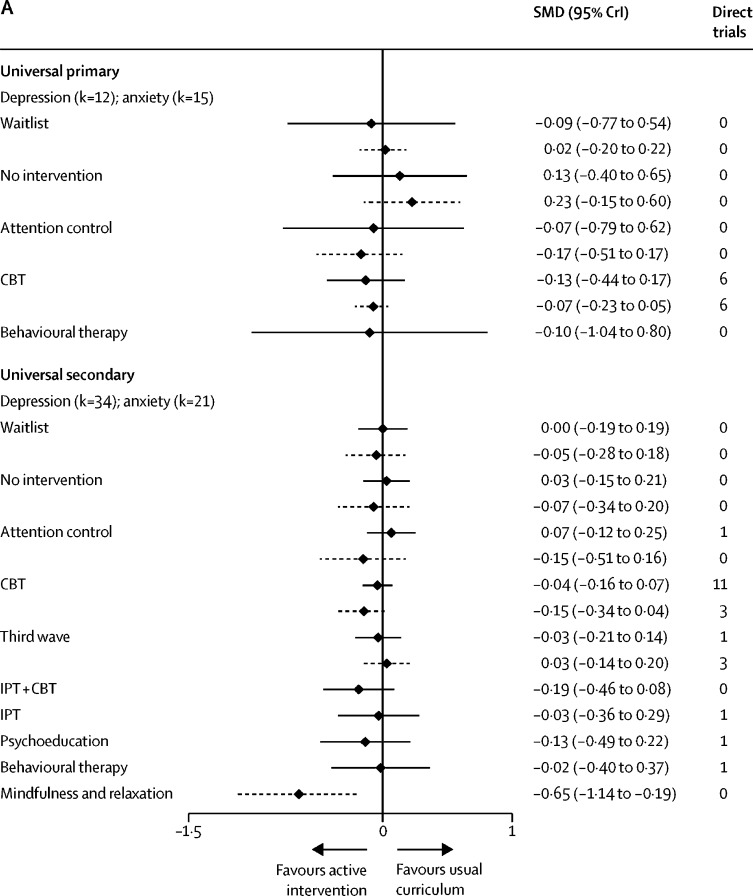
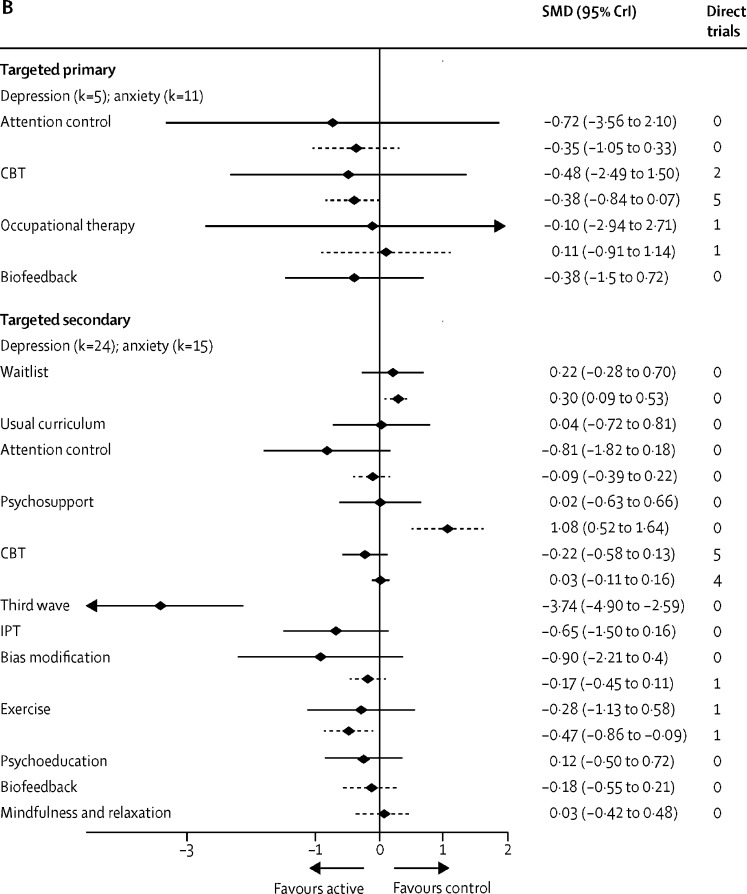
Findings: 1512 full-text articles were independently screened for inclusion by two reviewers, from which 137 studies of 56 620 participants were included. 20 studies were assessed as being at low risk of bias for both random sequence generation and allocation concealment. There was weak evidence to suggest that cognitive behavioural interventions might reduce anxiety in primary and secondary settings. In universal secondary settings, mindfulness and relaxation-based interventions showed a reduction in anxiety symptoms relative to usual curriculum (SMD -0·65, 95% credible interval -1·14 to -0·19). There was a lack of evidence to support any one type of intervention being effective to prevent depression in universal or targeted primary or secondary settings. Comparison-adjusted funnel plots suggest the presence of small-study effects for the universal secondary anxiety analysis. Network meta-analysis was not feasible for wellbeing or suicidal ideation or self-harm outcomes, and results are reported narratively.
Interpretation: Considering unclear risk of bias and probable small study effects for anxiety, we conclude there is little evidence that educational setting-based interventions focused solely on the prevention of depression or anxiety are effective. Future research could consider multilevel, systems-based interventions as an alternative to the downstream interventions considered here.
Funding: UK National Institute for Health Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Prevention versus intervention in school mental health.Lancet Psychiatry. 2019 Dec;6(12):969-971. doi: 10.1016/S2215-0366(19)30440-7. Epub 2019 Nov 14. Lancet Psychiatry. 2019. PMID: 31734107 No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2017. Global accelerated action for the health of adolescents (AA-HA!): guidance to support country implementation.
-
- Patton GC, Coffey C, Romaniuk H. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet. 2014;383:1404–1411. - PubMed
-
- Royal College of Psychiatrists . Royal College of Psychiatrists; London, UK: 2010. No health without public mental health: the case for action. Position Statement PS4/2010.
-
- Gore FM, Bloem PJ, Patton GC. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011;377:2093–2102. - PubMed
-
- Bor W, Dean AJ, Najman J, Hayatbakhsh R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust N Z J Psychiatry. 2014;48:606–616. - PubMed
