

Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial
- PMID: 31734701
- PMCID: PMC6865325
- DOI: 10.1001/jamacardio.2019.5006
Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial
Abstract
Importance: Guidelines recommend exercise training as a component of heart failure management. There are large disparities in access to rehabilitation, and introducing hybrid comprehensive telerehabilitation (HCTR) consisting of remote monitoring of training at patients' homes might be an appealing alternative.
Objective: To assess whether potential improvements in quality-of-life outcomes after a 9-week HCTR intervention in patients with heart failure translate into improvement in clinical outcomes during extended 12 to 24 months of follow-up, compared with usual care.
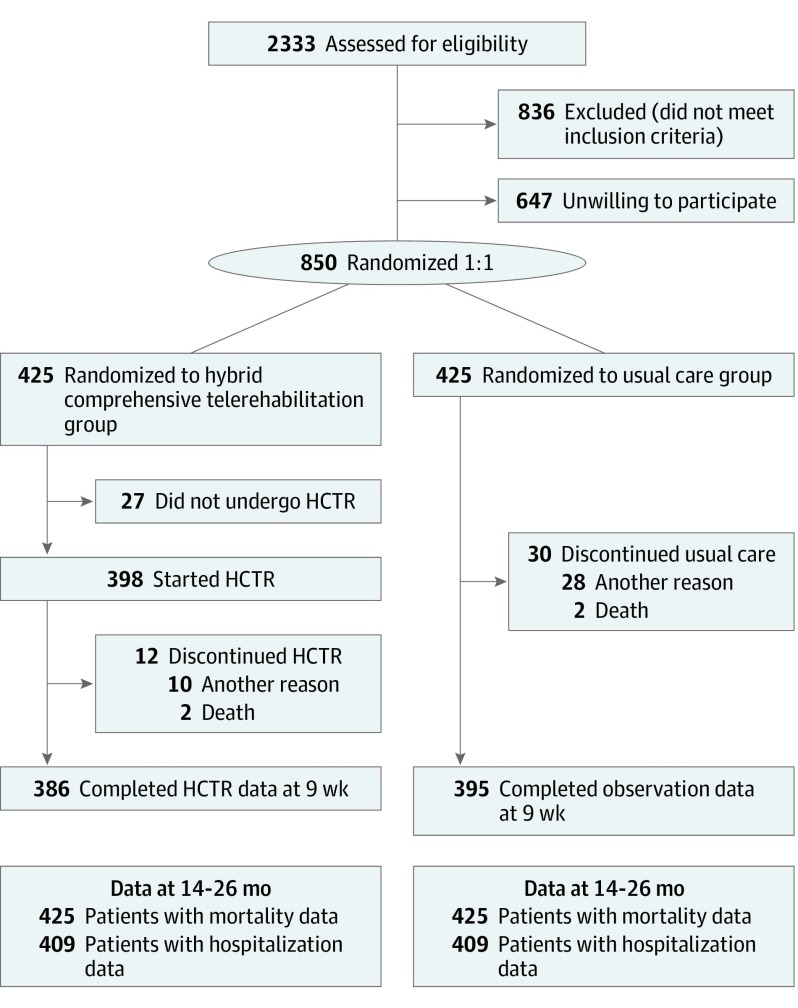
Design, setting, and participants: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) trial is a multicenter, prospective, open-label, parallel-group randomized clinical trial that enrolled 850 patients with heart failure up to 6 months after a cardiovascular hospitalization with New York Heart Association levels I, II, or III and left ventricular ejection fraction of 40% or less. Patients from 5 centers in Poland were randomized 1:1 to HCTR plus usual care or usual care only and followed up for 14 to 26 months after randomization.
Interventions: During the first 9 weeks, patients underwent either an HCTR program (1 week in hospital and 8 weeks at home) or usual care with observation. The HCTR intervention encompassed telecare, telerehabilitation, and remote monitoring of implantable devices. No intervention occurred in the remaining study period.
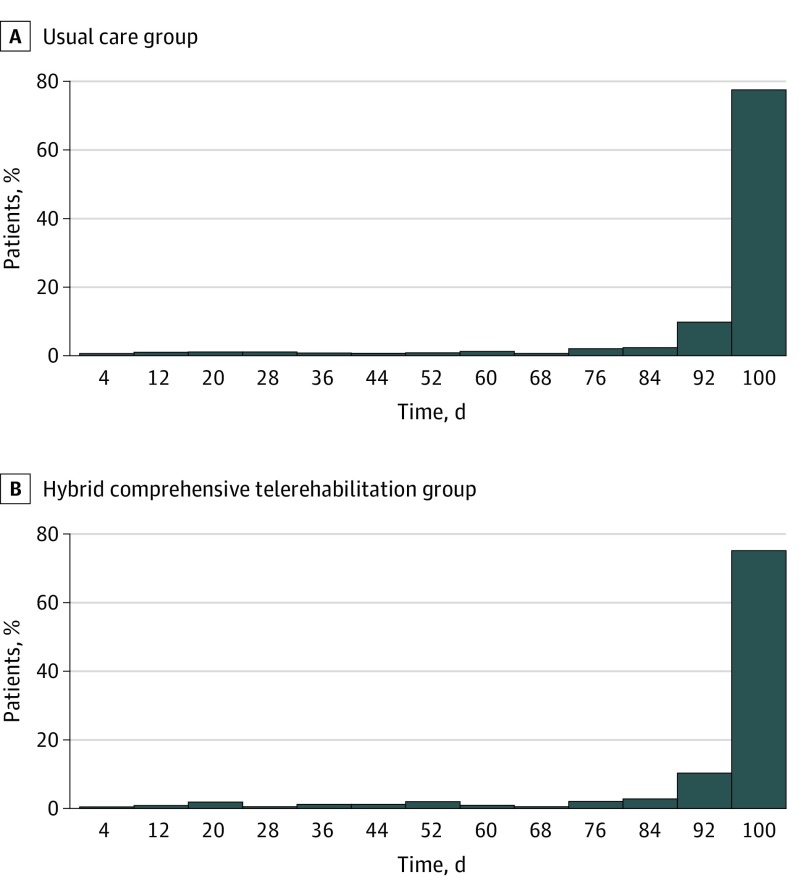
Main outcomes and measures: The percentage of days alive and out of the hospital from randomization through the end of follow-up at 14 to 26 months.
Results: A total of 850 patients were enrolled, with 425 randomized to the HCTR group (377 male patients [88.7%]; mean [SD] age, 62.6 [10.8] years) and 425 randomized to usual care (376 male patients [88.5%]; mean [SD] age, 62.2 [10.2] years). The HCTR intervention did not extend the percentage of days alive and out of the hospital. The mean (SD) days were 91.9 (19.3) days in the HCTR group vs 92.8 (18.3) days in the usual-care group, with the probability that HCTR extends days alive and out of the hospital equal to 0.49 (95% CI, 0.46-0.53; P = .74) vs usual care. During follow-up, 54 patients died in the HCTR arm and 52 in the usual-care arm, with mortality rates at 26 months of 12.5% vs 12.4%, respectively (hazard ratio, 1.03 [95% CI, 0.70-1.51]). There were also no differences in hospitalization rates (hazard ratio, 0.94 [95% CI, 0.79-1.13]). The HCTR intervention was effective at 9 weeks, significantly improving peak oxygen consumption (0.95 [95% CI, 0.65-1.26] mL/kg/min vs 0.00 [95% CI, -0.31 to 0.30] mL/kg/min; P < .001) and quality of life (Medical Outcome Survey Short Form-36 questionnaire score, 1.58 [95% CI, 0.74-2.42] vs 0.00 [95% CI, -0.84 to 0.84]; P = .008), and it was well tolerated, with no serious adverse events during exercise.
Conclusions and relevance: In this trial, the positive effects of a 9-week program of HCTR in patients with heart failure did not lead to the increase in percentage of days alive and out of the hospital and did not reduce mortality and hospitalization over a follow-up period of 14 to 26 months.
Trial registration: ClinicalTrials.gov identifier: NCT02523560.
Conflict of interest statement
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, et al. ; Authors/Task Force Members; Document Reviewers . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Eur J Heart Fail. 2016;18(8):891-975. doi:10.1002/ejhf.592 - DOI - PubMed
-
- Seferovic PM, Ponikowski P, Anker SD, et al. . Clinical practice update on heart failure 2019: pharmacotherapy, procedures, devices and patient management: an expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2019;21(10):1169-1186. Epub ahead of print. doi:10.1002/ejhf.1531 - DOI - PubMed
-
- Fletcher GF, Ades PA, Kligfield P, et al. ; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention . Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128(8):873-934. doi:10.1161/CIR.0b013e31829b5b44 - DOI - PubMed
-
- Thomas RJ, Beatty AL, Beckie TM, et al. . Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. J Am Coll Cardiol. 2019;74(1):133-153. doi:10.1016/j.jacc.2019.03.008 - DOI - PMC - PubMed
-
- Brignole M, Auricchio A, Baron-Esquivias G, et al. ; ESC Committee for Practice Guidelines (CPG); Document Reviewers . 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC), developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34(29):2281-2329. doi:10.1093/eurheartj/eht150 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
