

A phase I trial evaluating the safety and immunogenicity of a candidate tuberculosis vaccination regimen, ChAdOx1 85A prime - MVA85A boost in healthy UK adults
- PMID: 31735500
- PMCID: PMC6985898
- DOI: 10.1016/j.vaccine.2019.10.102
A phase I trial evaluating the safety and immunogenicity of a candidate tuberculosis vaccination regimen, ChAdOx1 85A prime - MVA85A boost in healthy UK adults
Abstract
Background: This phase I trial evaluated the safety and immunogenicity of a candidate tuberculosis vaccination regimen, ChAdOx1 85A prime-MVA85A boost, previously demonstrated to be protective in animal studies, in healthy UK adults.
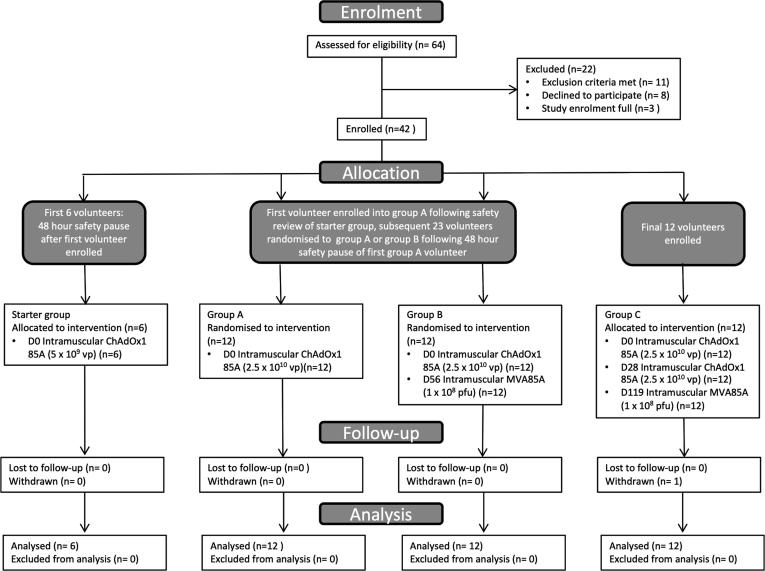
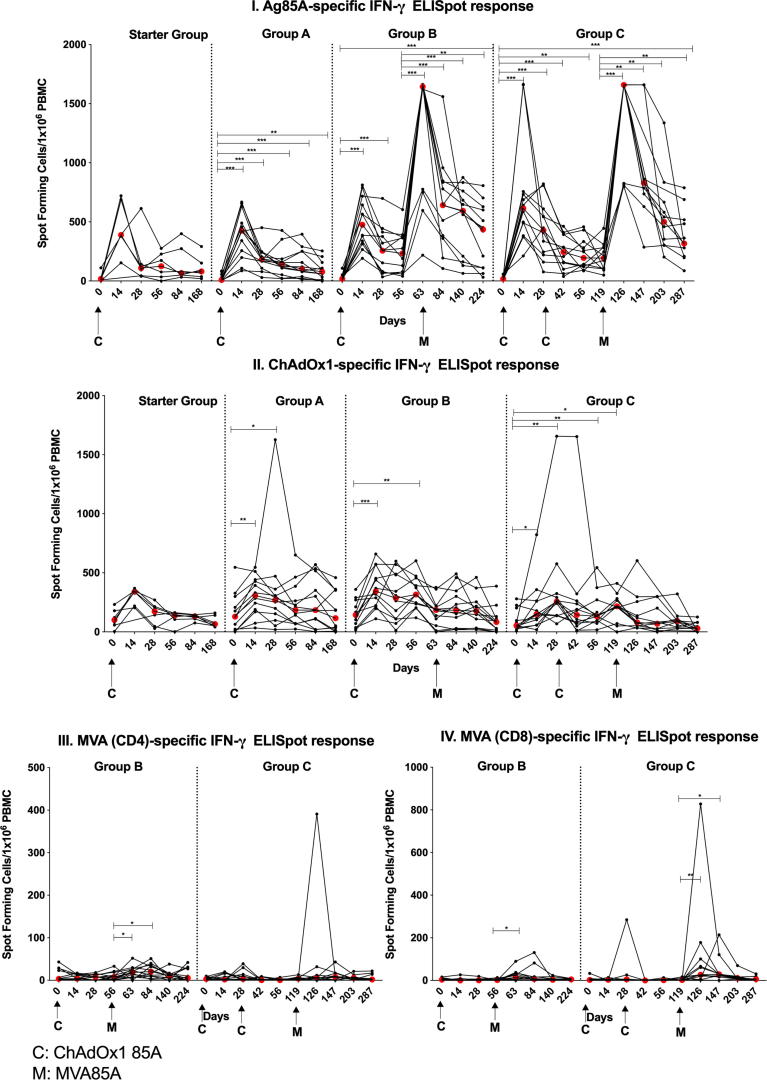
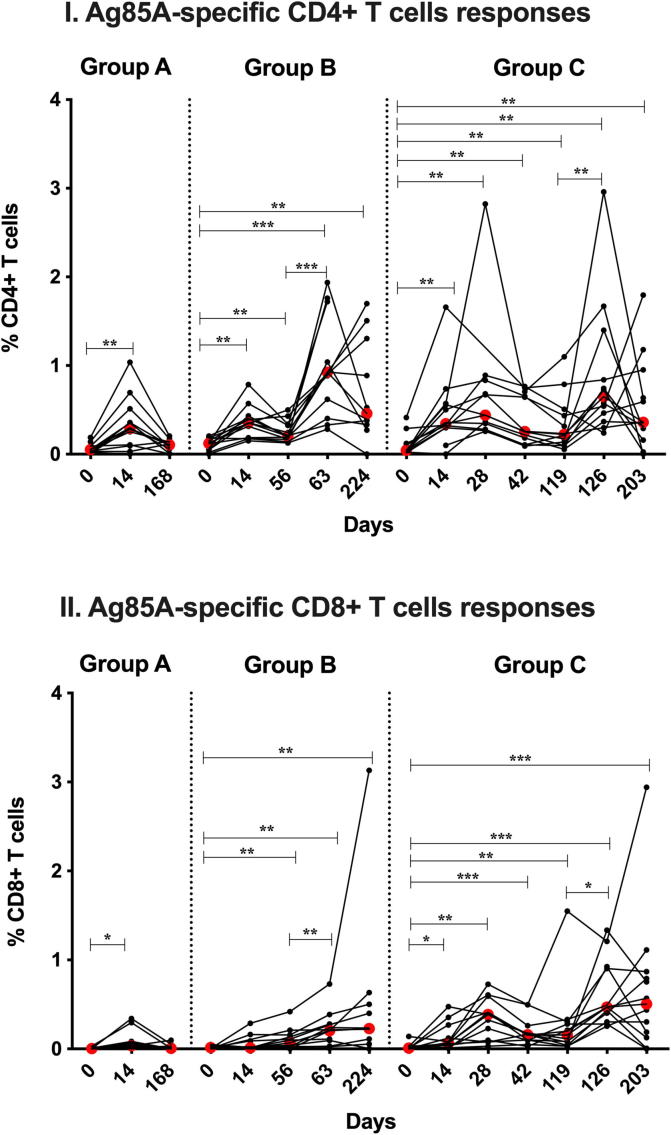
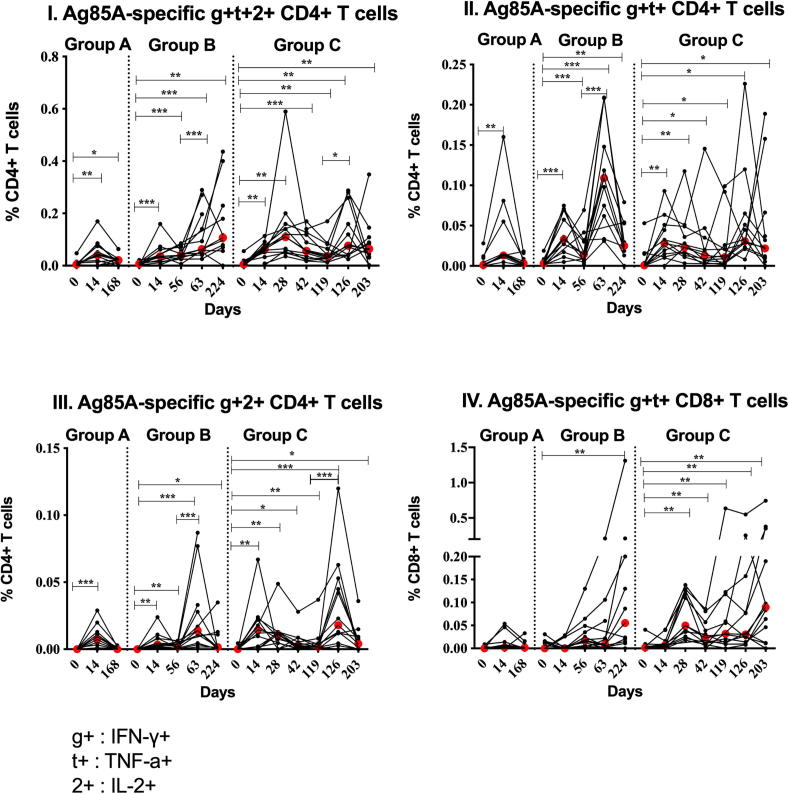
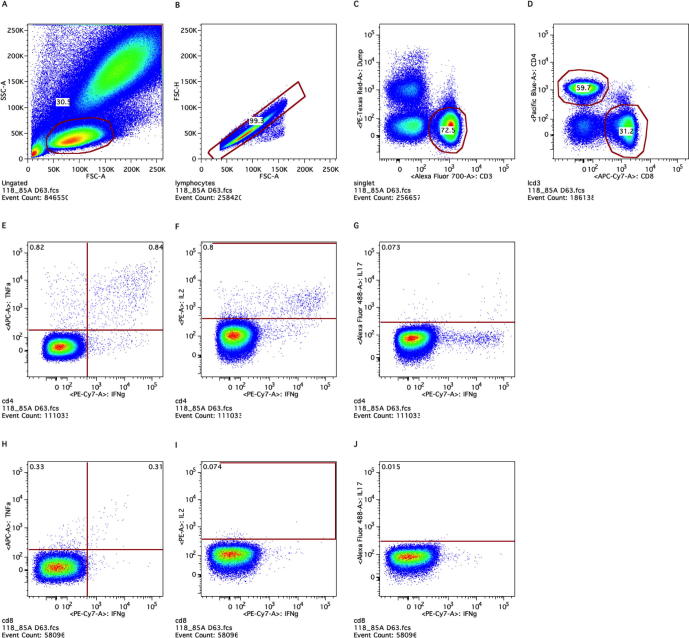
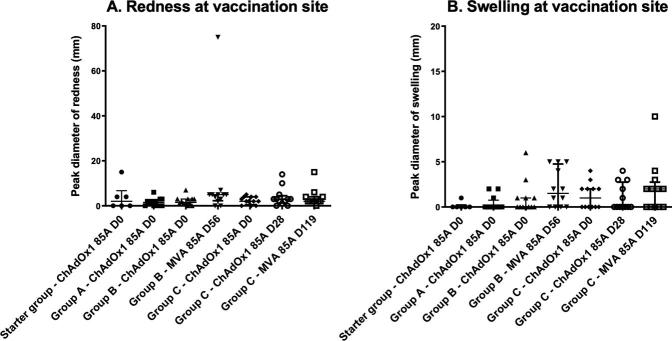
Methods: We enrolled 42 healthy, BCG-vaccinated adults into 4 groups: low dose Starter Group (n = 6; ChAdOx1 85A alone), high dose groups; Group A (n = 12; ChAdOx1 85A), Group B (n = 12; ChAdOx1 85A prime - MVA85A boost) or Group C (n = 12; ChAdOx1 85A - ChAdOx1 85A prime - MVA85A boost). Safety was determined by collection of solicited and unsolicited vaccine-related adverse events (AEs). Immunogenicity was measured by antigen-specific ex-vivo IFN-γ ELISpot, IgG serum ELISA, and antigen-specific intracellular IFN-γ, TNF-α, IL-2 and IL-17.
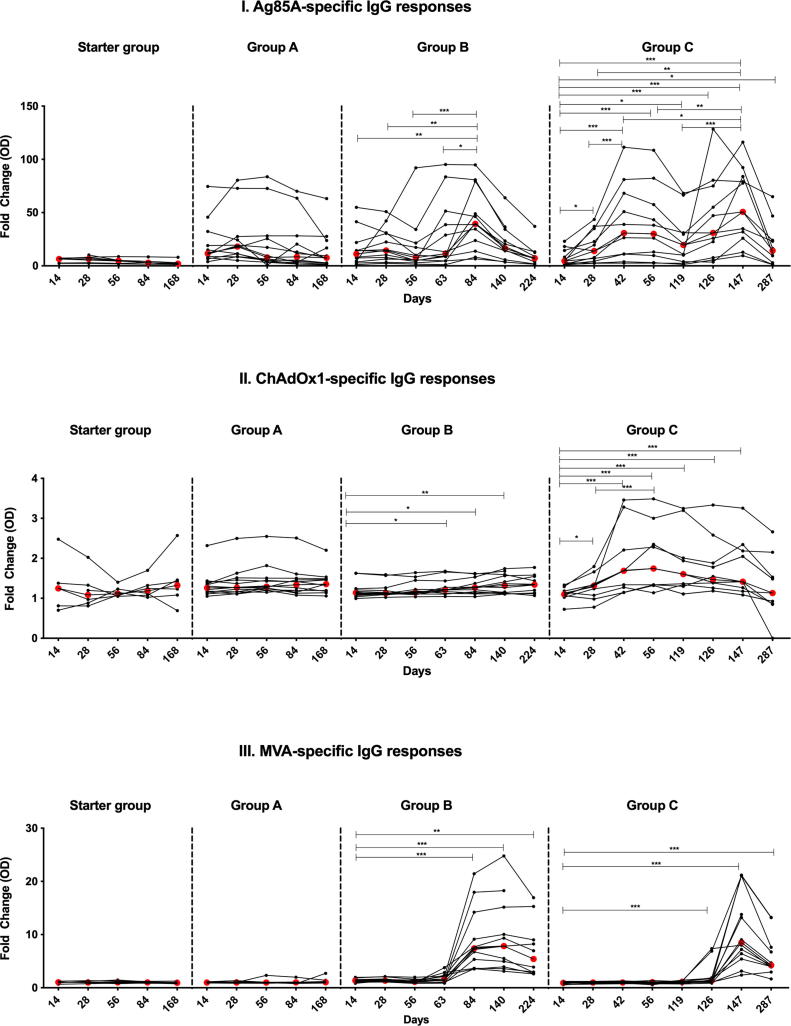
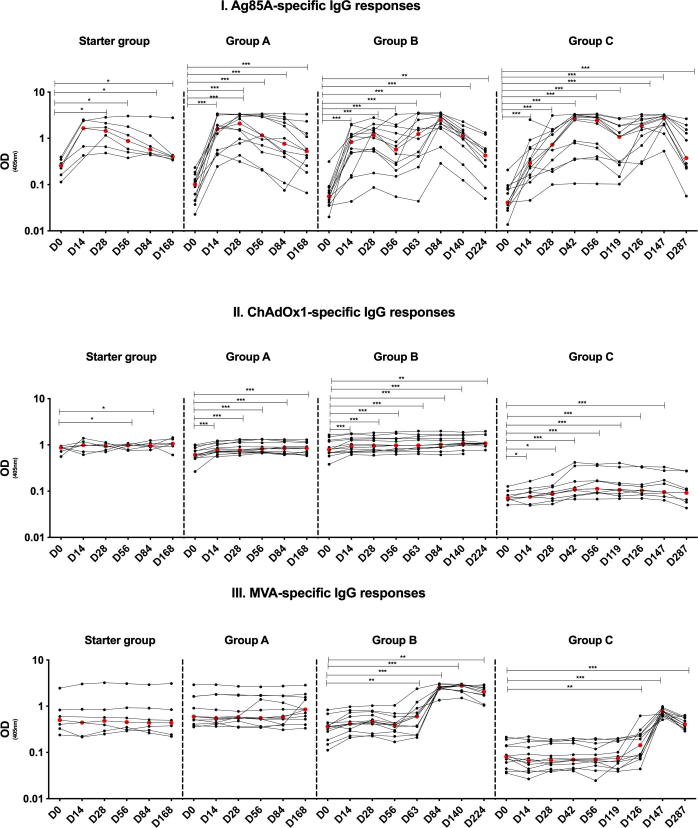
Results: AEs were mostly mild/moderate, with no Serious Adverse Events. ChAdOx1 85A induced Ag85A-specific ELISpot and intracellular cytokine CD4+ and CD8+ T cell responses, which were not boosted by a second dose, but were boosted with MVA85A. Polyfunctional CD4+ T cells (IFN-γ, TNF-α and IL-2) and IFN-γ+, TNF-α+ CD8+ T cells were induced by ChAdOx1 85A and boosted by MVA85A. ChAdOx1 85A induced serum Ag85A IgG responses which were boosted by MVA85A.
Conclusion: A ChAdOx1 85A prime - MVA85A boost is well tolerated and immunogenic in healthy UK adults.
Keywords: ChAdOx1 85A; Immunogenicity; MVA85A; Safety; Tuberculosis; Vaccine.
Copyright © 2019 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- WHO, Global tuberculosis report 2016; 2017.
-
- The Global Plan to End TB: The Paradigm Shift 2016–2020. Stop TB Partnership; 2016.
-
- Colditz G.A. Efficacy of BCG vaccine in the prevention of tuberculosis: meta-analysis of the published literature. JAMA. 1994;271(9):698–702. - PubMed
-
- Trunz B.B., Fine P., Dye C. Effect of BCG vaccination on childhood tuberculous meningitis and miliary tuberculosis worldwide: a meta-analysis and assessment of cost-effectiveness. The Lancet. 2006;367(9517):1173–1180. - PubMed
-
- Rodrigues L.C., Diwan V.K., Wheeler J.G. Protective effect of BCG against tuberculous meningitis and miliary tuberculosis: a meta-analysis. Int J Epidemiol. 1993;22(6):1154–1158. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
