

Identification of an immunotherapy-responsive molecular subtype of bladder cancer
- PMID: 31735557
- PMCID: PMC6921227
- DOI: 10.1016/j.ebiom.2019.10.058
Identification of an immunotherapy-responsive molecular subtype of bladder cancer
Abstract
Background: Although various molecular subtypes of bladder cancer (BC) have been investigated, most of these studies have focused on muscle-invasive BC (MIBC). A few studies have investigated non-muscle-invasive BC (NMIBC) or NMIBC and MIBC together, but none has classified progressive NMIBC or immune checkpoint inhibitor (ICI)-based therapeutic responses in early-stage BC patients.
Methods: A total of 1,934 samples from seven patient cohorts were used. We performed unsupervised hierarchical clustering to stratify patients into distinct subgroups and constructed a classifier by applying SAM/PAM algorithms. We then investigated the association between molecular subtypes and immunotherapy responsiveness using various statistical methods.
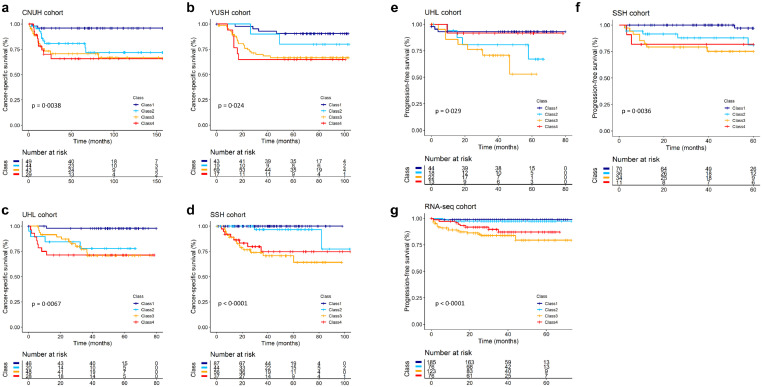
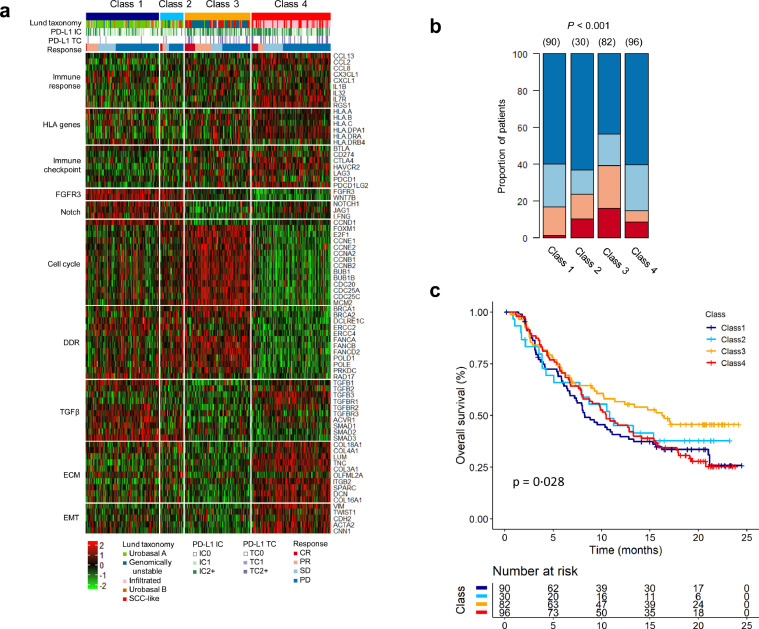
Findings: We explored large-scale genomic datasets encompassing NMIBC and MIBC, redefining four distinct molecular subtypes, including a subgroup containing progressive NMIBC and MIBC with poor prognosis that would benefit from ICI treatment. This subgroup showed poor progression-free survival with the distinct features of high mutation load, activated cell cycle, and inhibited TGFβ signalling. Importantly, we verified that BC patients with this subtype were significantly responsive to an anti-PD-L1 agent in the IMvigor210 cohort.
Interpretation: Our results reveal an immunotherapeutic option for ICI treatment of highly progressive NMIBC and MIBC with poor prognosis.
Funding: This research was supported by the National Research Foundation of Korea grant funded by the Korean government, a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea, and a grant from the KRIBB Research Initiative Program.
Keywords: Bladder cancer; Disease progression; Genomic signature; Immunotherapy; Subtype.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Molecular Subtypes of Urothelial Bladder Cancer: Results from a Meta-cohort Analysis of 2411 Tumors.Eur Urol. 2019 Mar;75(3):423-432. doi: 10.1016/j.eururo.2018.08.027. Epub 2018 Sep 10. Eur Urol. 2019. PMID: 30213523
-
Predictive value of progression-related gene classifier in primary non-muscle invasive bladder cancer.Mol Cancer. 2010 Jan 8;9:3. doi: 10.1186/1476-4598-9-3. Mol Cancer. 2010. PMID: 20059769 Free PMC article.
-
Intratumoral IL22-producing cells define immunoevasive subtype muscle-invasive bladder cancer with poor prognosis and superior nivolumab responses.Int J Cancer. 2020 Jan 15;146(2):542-552. doi: 10.1002/ijc.32715. Epub 2019 Oct 23. Int J Cancer. 2020. PMID: 31584197
-
The evolution of bladder cancer genomics: What have we learned and how can we use it?Urol Oncol. 2018 Jul;36(7):313-320. doi: 10.1016/j.urolonc.2018.02.017. Epub 2018 Mar 21. Urol Oncol. 2018. PMID: 29573965 Review.
-
Biomarkers for precision medicine in bladder cancer.Int J Clin Oncol. 2017 Apr;22(2):207-213. doi: 10.1007/s10147-016-1068-8. Epub 2016 Nov 29. Int J Clin Oncol. 2017. PMID: 27896485 Review.
Cited by
-
An integrated multi-omics analysis identifies prognostic molecular subtypes of non-muscle-invasive bladder cancer.Nat Commun. 2021 Apr 16;12(1):2301. doi: 10.1038/s41467-021-22465-w. Nat Commun. 2021. PMID: 33863885 Free PMC article.
-
Development of an Immune-Related Risk Signature for Predicting Prognosis in Lung Squamous Cell Carcinoma.Front Genet. 2020 Aug 28;11:978. doi: 10.3389/fgene.2020.00978. eCollection 2020. Front Genet. 2020. PMID: 33005178 Free PMC article.
-
Identification of an Immune-Related Prognostic Signature Associated With Immune Infiltration in Melanoma.Front Genet. 2020 Aug 28;11:1002. doi: 10.3389/fgene.2020.01002. eCollection 2020. Front Genet. 2020. PMID: 33005180 Free PMC article.
-
Identification of an immune gene-associated prognostic signature in patients with bladder cancer.Cancer Gene Ther. 2022 May;29(5):494-504. doi: 10.1038/s41417-022-00438-5. Epub 2022 Feb 15. Cancer Gene Ther. 2022. PMID: 35169299
-
IGF2BP3 prevent HMGB1 mRNA decay in bladder cancer and development.Cell Mol Biol Lett. 2024 Mar 19;29(1):39. doi: 10.1186/s11658-024-00545-1. Cell Mol Biol Lett. 2024. PMID: 38504159 Free PMC article.
References
-
- Ferlay J., Soerjomataram I., Dikshit R. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. - PubMed
-
- Jordan B., Meeks J.J. T1 bladder cancer: current considerations for diagnosis and management. Nat Rev Urol. 2019;16(1):23–34. - PubMed
-
- Alfred Witjes J., Lebret T., Comperat E.M. Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol. 2017;71(3):462–475. - PubMed
-
- US National Library of Medicine. Atezolizumab in treating patients with recurrent BCG-unresponsive non-muscle invasive bladder cancer [Internet]. [cited 2019 May 9] Available from: https://ClinicalTrials.gov/show/NCT02844816.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
