

Metachronous Pancreatic Ductal Adenocarcinoma with Adjacent Serous Cystadenoma that Was Preoperatively Diagnosed by EUS-FNA: A Case Report and Review of the Literature
- PMID: 31735797
- PMCID: PMC7086322
- DOI: 10.2169/internalmedicine.3912-19
Metachronous Pancreatic Ductal Adenocarcinoma with Adjacent Serous Cystadenoma that Was Preoperatively Diagnosed by EUS-FNA: A Case Report and Review of the Literature
Abstract
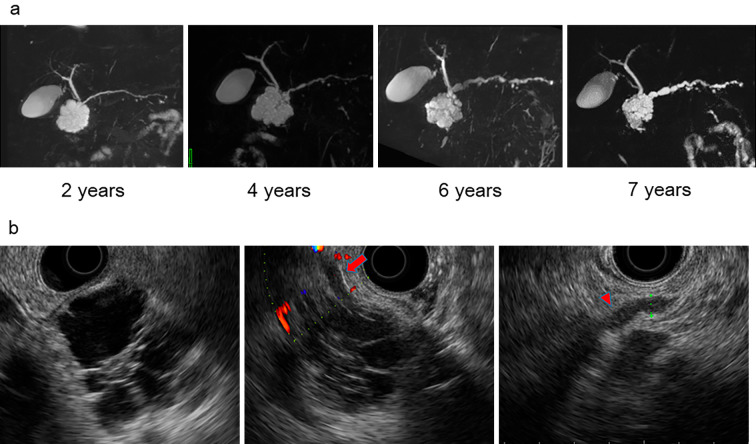
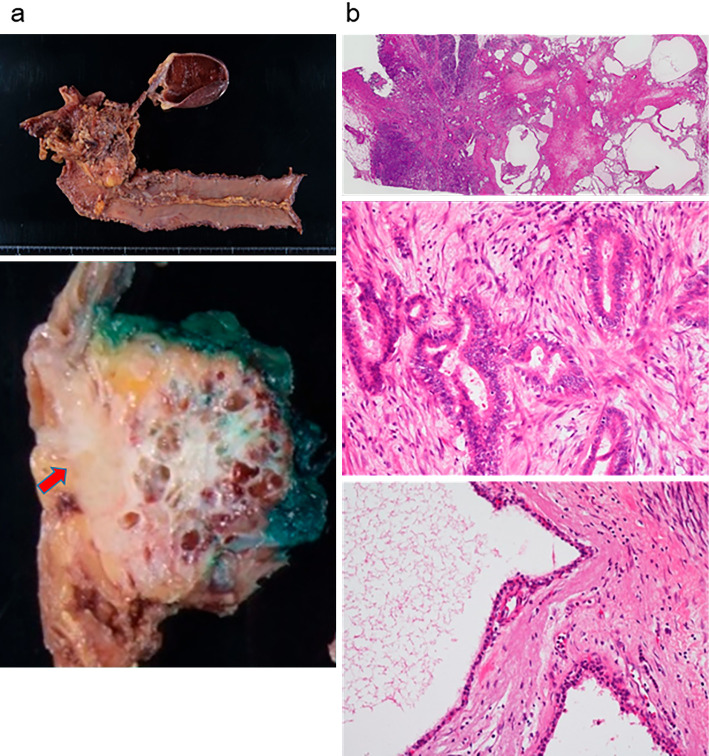
Pancreatic serous cystic neoplasms (SCNs), such as serous cystadenoma (SCA), are generally recognized as benign because malignant counterparts of SCNs have been extremely rare. In clinical practice, pancreatic cystic neoplasms diagnosed as SCNs have been managed by conservative observation, as long as the patients remained asymptomatic. We herein report a case of metachronous ductal adenocarcinoma that was discovered during long-term follow-up of SCN and review the related literature. To our knowledge, this was the first reported case of the local presence of ductal adenocarcinoma adjacent to SCA that was preoperatively diagnosed by endoscopic ultrasound-guided fine-needle aspiration.
Keywords: diffusion-weighted magnetic resonance image (DWI); endoscopic ultrasound-guided fine needle aspiration (EUS-FNA); pancreatic ductal adenocarcinoma (PDAC); serous cystadenoma (SCA); serous cystic neoplasm (SCN).
Conflict of interest statement
Figures





Similar articles
-
High Diagnostic Yield of Fine Needle Biopsy for Pancreatic Serous Cystadenomas-A Multicenter Study.Pancreas. 2025 Apr 1;54(4):e349-e352. doi: 10.1097/MPA.0000000000002442. Pancreas. 2025. PMID: 39626196
-
Serous cystadenoma of the pancreas: limitations and pitfalls of endoscopic ultrasound-guided fine-needle aspiration biopsy.Cancer. 2008 Apr 25;114(2):102-10. doi: 10.1002/cncr.23346. Cancer. 2008. PMID: 18260088
-
Coexisting pancreatic serous cystadenoma and pancreatic ductal adenocarcinoma: A cytological-pathologic correlation with literature review.Ann Diagn Pathol. 2019 Oct;42:87-91. doi: 10.1016/j.anndiagpath.2019.07.006. Epub 2019 Jul 27. Ann Diagn Pathol. 2019. PMID: 31382079 Review.
-
Complications of endoscopic ultrasound fine needle aspiration on pancreatic cystic lesions: final results from a large prospective multicenter study.Dig Liver Dis. 2014 Jan;46(1):41-4. doi: 10.1016/j.dld.2013.08.134. Epub 2013 Sep 17. Dig Liver Dis. 2014. PMID: 24054767
-
[Differential diagnosis of pancreatic lesions using endoscopic ultrasound].Z Gastroenterol. 2008 Jun;46(6):601-17. doi: 10.1055/s-2008-1027523. Z Gastroenterol. 2008. PMID: 18537088 Review. German.
Cited by
-
Concomitant occurrence of pancreatic cancer during long-term follow-up for serous neoplasms.J Med Ultrason (2001). 2023 Jul;50(3):451-452. doi: 10.1007/s10396-023-01327-6. Epub 2023 May 30. J Med Ultrason (2001). 2023. PMID: 37249692 No abstract available.
References
-
- Hruban RH, Pitman MB, Klimstra D. Tumors of the Pancreas. Atlas of Tumor Pathology, 4th series, fascicle 6. Amer Registry of Pathology, Silver Spring, MD, 2007: 43-55.
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. Serous neoplasms of the pancreas. In: WHO classification of tumours of the digestive system. 4th Ed. World Health Organization, Lyon, 2010: 296-299.
-
- Compagno J, Oertel JE. Microcystic adenomas of the pancreas (glycogen-rich cystadenomas): a clinicopathologic study of 34 cases. Am J Clin Pathol 69: 289-298, 1978. - PubMed
-
- Hodgkinson DJ, ReMine WH, Weiland LH. Pancreatic cystadenoma. A clinicopathologic study of 45 cases. Arch Surg 113: 512-519, 1978. - PubMed
-
- Kimura W, Moriya T, Hirai I, et al. . Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 41: 380-387, 2012. - PubMed