

Influence of Foetal Macrosomia on the Neonatal and Maternal Birth Outcome
- PMID: 31736508
- PMCID: PMC6846738
- DOI: 10.1055/a-0880-6182
Influence of Foetal Macrosomia on the Neonatal and Maternal Birth Outcome
Abstract
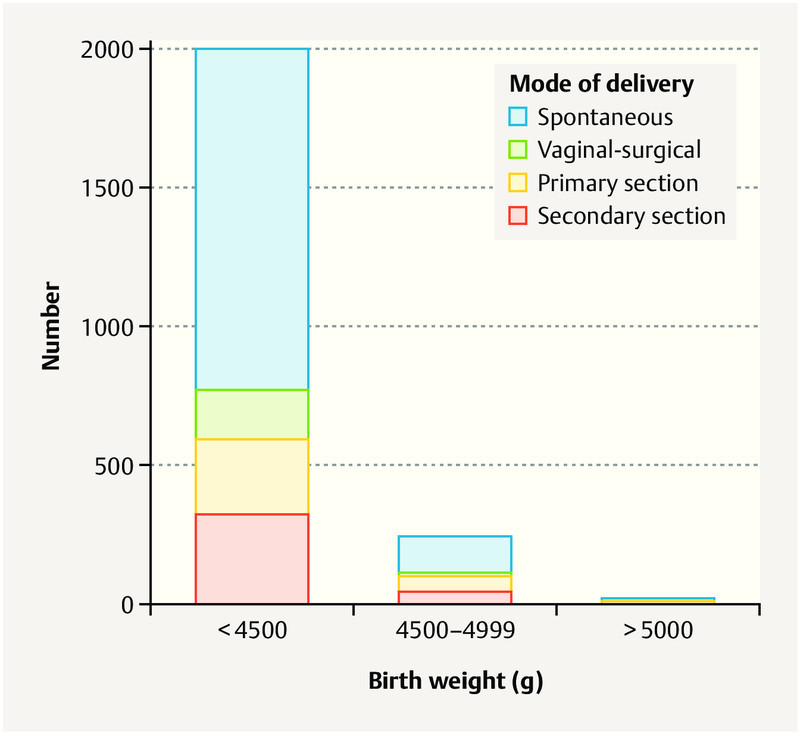
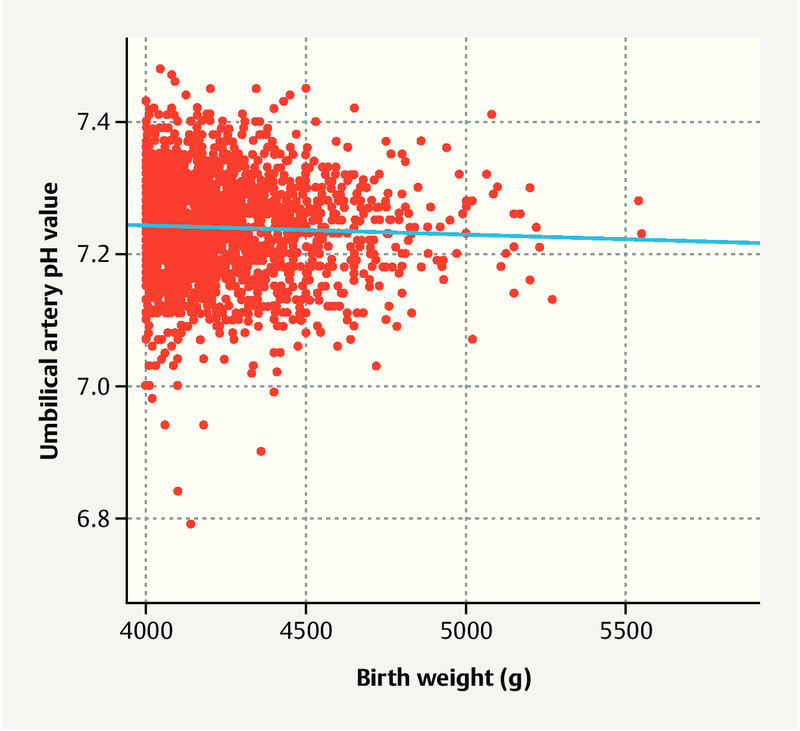
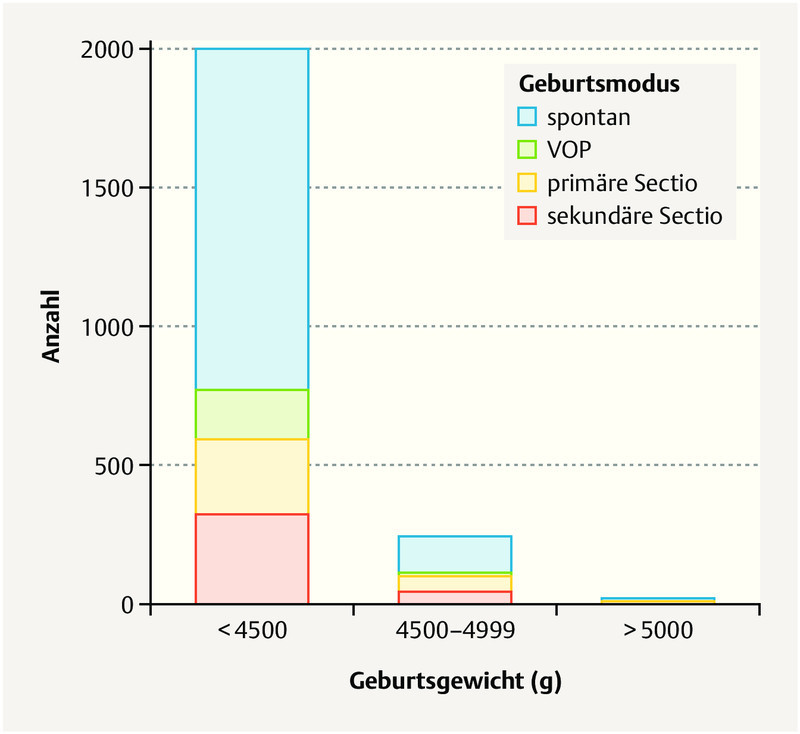
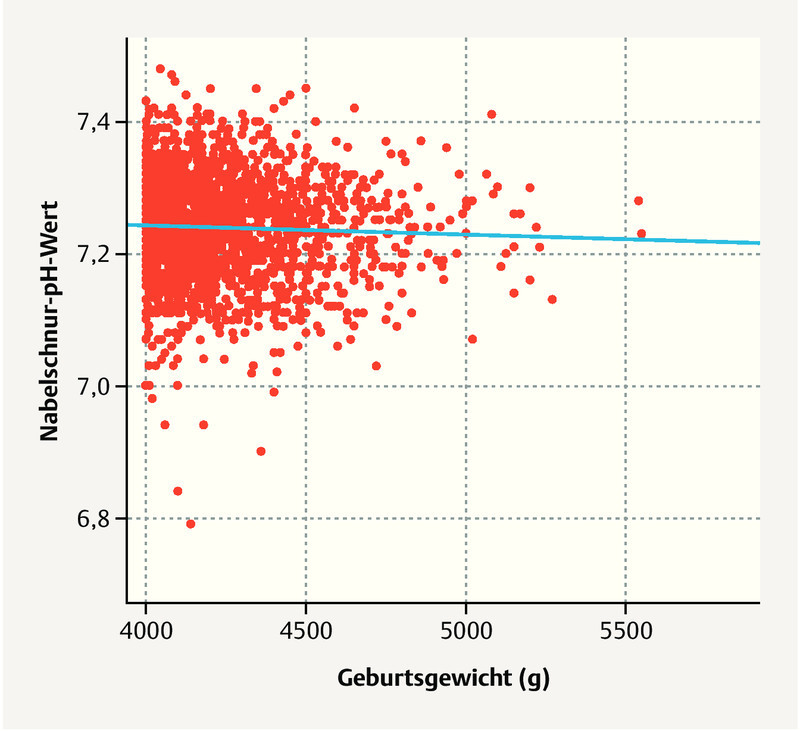
Introduction Foetal macrosomia is associated with various obstetrical complications and is a common reason for inductions and primary or secondary Caesarean sections. The objective of this study is the generation of descriptive data on the mode of delivery and on maternal and foetal complications in the case of foetal macrosomia. The causes and consequences of foetal macrosomia as well as the rate of shoulder dystocia are examined in relation to the severity of the macrosomia. Patients The study investigated all singleton births ≥ 37 + 0 weeks of pregnancy with a birth weight ≥ 4000 g at the Charité University Medicine Berlin (Campus Mitte 2001 - 2017, Campus Virchow Klinikum 2014 - 2017). Results 2277 consecutive newborns (birth weight 4000 - 4499 g [88%], 4500 - 4999 g [11%], ≥ 5000 g [1%]) were included. Maternal obesity and gestational diabetes were more common in the case of newborns weighing ≥ 4500 g than newborns weighing 4000 - 4499 g (p = 0.001 and p < 0.001). Women with newborns ≥ 5000 g were more often ≥ 40 years of age (p = 0.020) and multipara (p = 0.025). The mode of delivery was spontaneous in 60% of cases, vaginal-surgical in 9%, per primary section in 14% and per secondary section in 17%. With a birth weight ≥ 4500 g, a vaginal delivery was more rare (p < 0.001) and the rate of secondary sections was increased (p = 0.011). Women with newborns ≥ 4500 g suffered increased blood loss more frequently (p = 0.029). There was no significant difference with regard to the rate of episiotomies or serious birth injuries. Shoulder dystocia occurred more frequently at a birth weight of ≥ 4500 g (5 vs. 0.9%, p = 0.000). Perinatal acidosis occurred in 2% of newborns without significant differences between the groups. Newborns ≥ 4500 g were transferred to neonatology more frequently (p < 0.001). Conclusion An increased birth weight is associated with an increased maternal risk and an increased rate of primary and secondary sections as well as shoulder dystocia; no differences in the perinatal outcome between newborns with a birth weight of 4000 - 4499 g and ≥ 4500 g were seen. In our collective, a comparably low incidence of shoulder dystocia was seen. In the literature, the frequency is indicated with a large range (1.9 - 10% at 4000 - 4499 g, 2.5 - 20% at 4500 - 5000 g and 10 - 20% at ≥ 5000 g). One possible cause for the low rate could be the equally low prevalence of gestational diabetes in our collective. A risk stratification of the pregnant women (e.g. avoidance of vacuum extraction, taking gestational diabetes into account during delivery planning) is crucial. If macrosomia is presumed, it is recommended that delivery take place at a perinatal centre in the presence of a specialist physician, due to the increased incidence of foetal and maternal complications.
Keywords: foetal macrosomia; gestational diabetes; shoulder dystocia.
Conflict of interest statement
Conflict of Interest/Interessenkonflikt The authors declare that they have no conflict of interest./Die Autoren geben an, dass kein Interessenkonflikt besteht.
Figures
References
-
- American College of Obstetricians and Gynecologistsʼ Committee on Practice Bulletins—Obstetrics . Practice Bulletin No. 173: Fetal Macrosomia. Obstet Gynecol. 2016;128:e195–e209. - PubMed
-
- Zhang X, Decker A, Platt R W. How big is too big? The perinatal consequences of fetal macrosomia. Am J Obstet Gynecol. 2008;198:5170–5.17E8. - PubMed
-
- Boulet S L, Alexander G R, Salihu H M. Macrosomic births in the united states: determinants, outcomes, and proposed grades of risk. Am J Obstet Gynecol. 2003;188:1372–1378. - PubMed
-
- Tian C, Hu C, He X. Excessive weight gain during pregnancy and risk of macrosomia: a meta-analysis. Arch Gynecol Obstet. 2016;293:29–35. - PubMed
LinkOut - more resources
Full Text Sources