

Comparison between thoracoscopic and open approaches in thymoma resection
- PMID: 31737299
- PMCID: PMC6837992
- DOI: 10.21037/jtd.2019.09.85
Comparison between thoracoscopic and open approaches in thymoma resection
Abstract
Background: To investigate the feasibility and indications of video-assisted thoracic surgery (VATS) in thymoma resection.
Methods: The clinical data of 103 patients undergoing thymoma resection via different approaches [including conventional lateral thoracotomy approach (LTA) in 41 cases, median sternotomy approach (MSA) in 40 cases, and right-sided VATS in 22 cases] were analyzed. Among them, 59, 13, 25, and 6 patients were in Masaoka stage I, II, III, and IV, respectively. Myasthenia gravis (MG) was also found in 54 cases. The patients were followed up for postoperative survival and the improvement in MG. The prognostic indicators of patients undergoing thymoma resection via different surgical approaches (i.e., LTA, MSA, and VATS) were statistically analyzed.
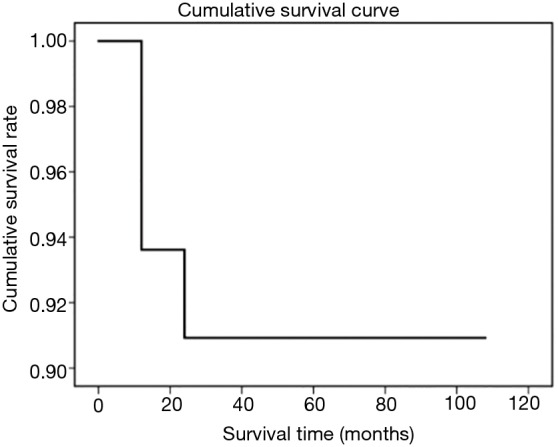
Results: Eight of 103 patients died. Six patients underwent unilateral sacral nerve resection, among whom 4 patients developed respiratory dysfunction, and 3 died. Two patients died of MG after surgery, 1 patient died of tumor recurrence and metastasis, 1 patient died of heart disease, and the cause of death was unknown in the remaining patient. The drainage time was shorter in VATS group than in open groups, along with smaller tumor size. The VATS group also had shorter hospital stay in the whole series and the subgroup without accompanying MG. The improvement in MG showed no significant difference among the three surgical groups. Both 5- and 10-year survival rates were 91% in the entire cohort.
Conclusions: VATS is like a conventional surgeries for improving MG in thymoma patients with accompanying MG. VATS resection can still be considered for thymoma that only invades the mediastinal pleura. For thymomas that have intact capsules and have not invaded mediastinal pleura, MSA surgery shall be performed to ensure patient safety if the anteroposterior diameters of the tumors are large and the masses have produced severe compression of the innominate vein, even if the tumors are still in the Masaoka stage II. For thymomas with large left-to-right diameters and with most parts of the tumors located in the left thoracic cavity, a left-sided approach (either VATS or an open approach) may be used in the absence of MG; if MG accompanies the condition, an MT approach or a bilateral VATS may be considered. In patients with unilateral pericardial phrenic nerve and/or local pericardial involvement, right-sided VATS thymectomy may be considered for thymomas located at the right side and bilateral VATS surgery can be performed for tumors located at the left side. In summary, VATS is feasible for the treatment of thymoma complicated by MG. VATS can be performed in patients with Masaoka stage I, II and (a certain portion of) III thymoma; for some patients with Masaoka stage II thymoma, especially those with compression of the innominate vein, the use of VATS should be cautious.
Keywords: Thymoma; myasthenia gravis (MG); video-assisted thoracic surgery (VATS).
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
LinkOut - more resources
Full Text Sources