

Dynamic Contributions of Slow Wave Sleep and REM Sleep to Cognitive Longevity
- PMID: 31737466
- PMCID: PMC6857934
- DOI: 10.1007/s40675-018-0131-6
Dynamic Contributions of Slow Wave Sleep and REM Sleep to Cognitive Longevity
Abstract
Purpose of review: The purpose of this paper was to address how sleep changes with aging, with the broader goal of informing how REM sleep and slow wave activity mechanisms interact to promote cognitive longevity.
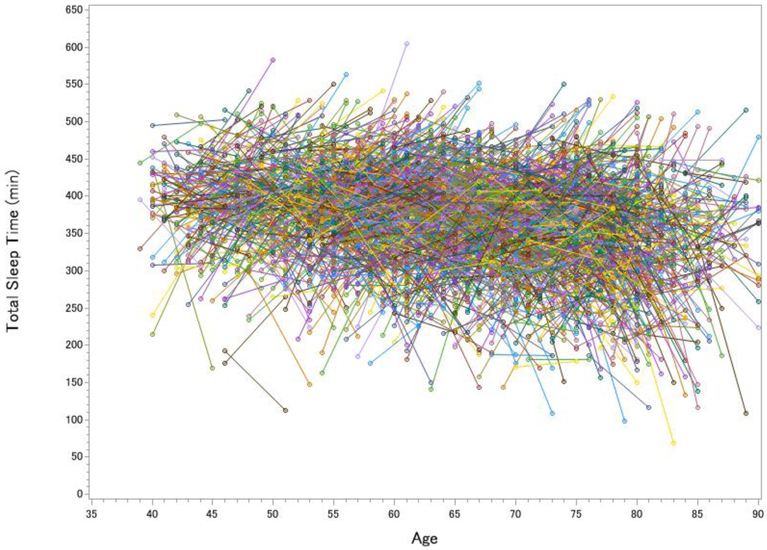
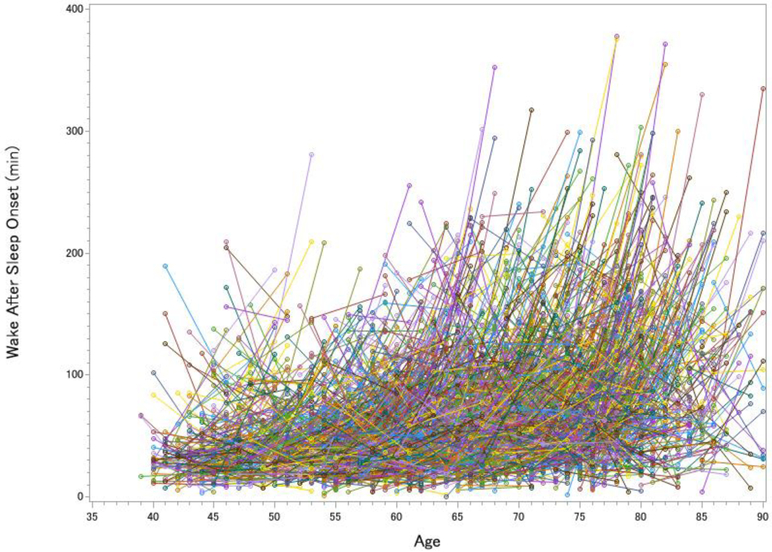
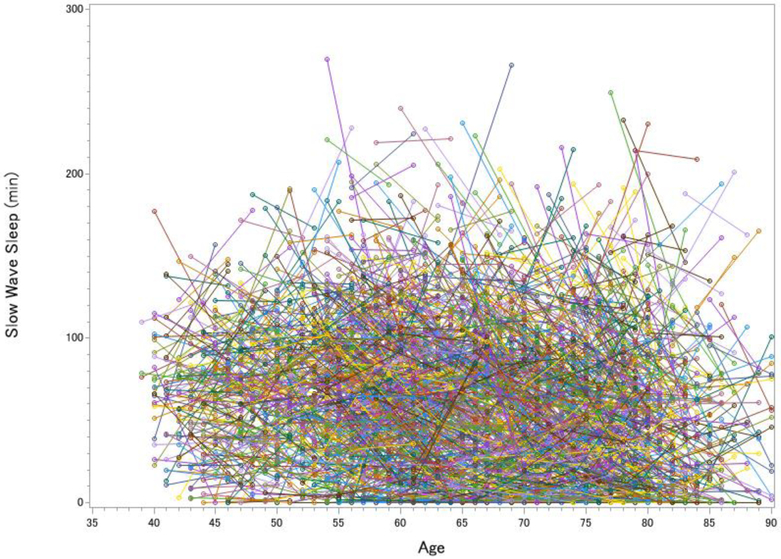
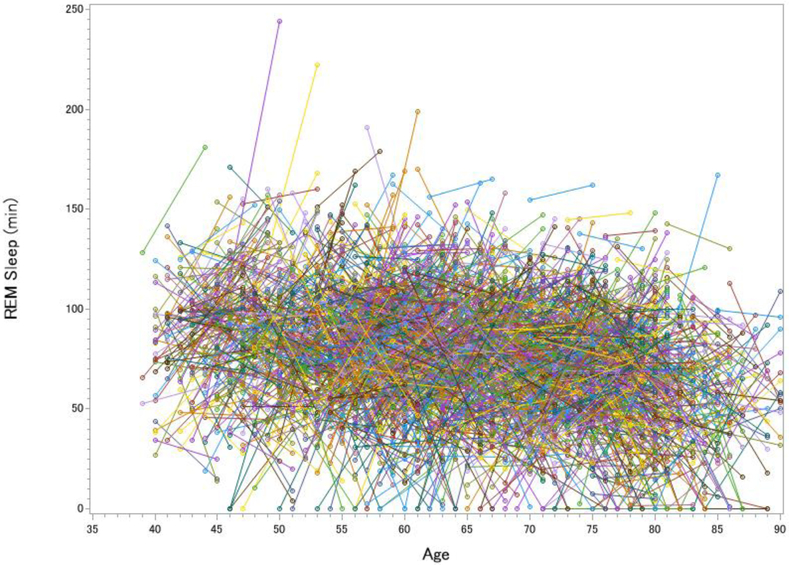
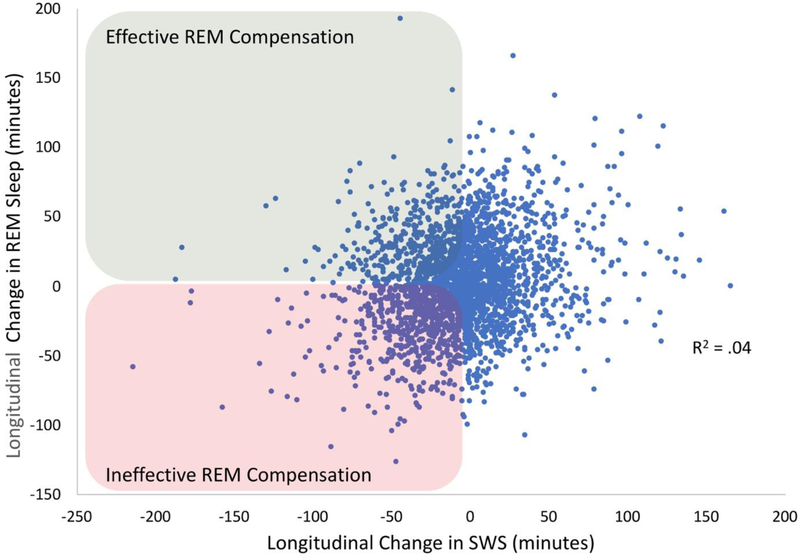
Recent findings: We conducted novel analyses based on the National Sleep Research Resource database. Over approximately five years, middle-to-older aged adults, on average, showed dramatically worse sleep fragmentation, a steady decrease in slow wave sleep, and yet a small increase in REM sleep. Averaging across participants, however, masked a major theme: Individuals differ substantially in their longitudinal trajectories for specific components of sleep. We considered this individual variability in light of recent theoretical and empirical work that has shown disrupted sleep and decreased slow wave activity to impair frontal lobe restoration, glymphatic system functioning, and memory consolidation. Based on multiple recent longitudinal studies, we contend that preserved or enhanced REM sleep may compensate for otherwise disrupted sleep in advancing age.
Summary: The scientific community has often debated whether slow wave activity or REM sleep mechanisms are more important to cognitive aging. We propose that a more fruitful approach for future work will be to investigate how REM and slow wave processes dynamically interact to affect cognitive longevity.
Keywords: National Sleep Research Resource; dementia; memory consolidation; older adults; sequential hypothesis; sleep spindles.
Conflict of interest statement
Conflict of Interest Michael K. Scullin reports a grant for research on memory and aging by NIH AG053161. Chenlu Gao declares no potential conflicts of interest.
Figures
References
-
-
Jackson JH. The Croonian lectures on evolution and dissolution of the nervous system. BMJ 1884;1:703–7.
• He theorized about dissociable, interactive sleep-based cognitive processes one year before Ebbinghaus’ seminal work on the forgetting curve, and nearly 70 years before the discovery of sleep stages.
-
-
- Global Council on Brain Health. The brain-sleep connection: GCBH recommendations on sleep and brain health. American Association of Retired Persons. 2016. https://www.aarp.org/content/dam/aarp/health/healthy-living/2017/01/gcbh.... Accessed 7 Sept 2018.
-
- Miles LE, Dement WC. Sleep and aging. Sleep 1980;3(2):1–220. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials