

Incidence and Risk Factors of Early Onset Neonatal AKI
- PMID: 31738181
- PMCID: PMC6390916
- DOI: 10.2215/CJN.03670318
Incidence and Risk Factors of Early Onset Neonatal AKI
Abstract
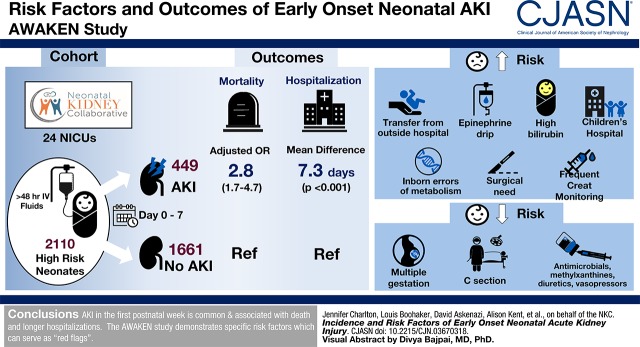
Background and objectives: Neonatal AKI is associated with poor short- and long-term outcomes. The objective of this study was to describe the risk factors and outcomes of neonatal AKI in the first postnatal week.
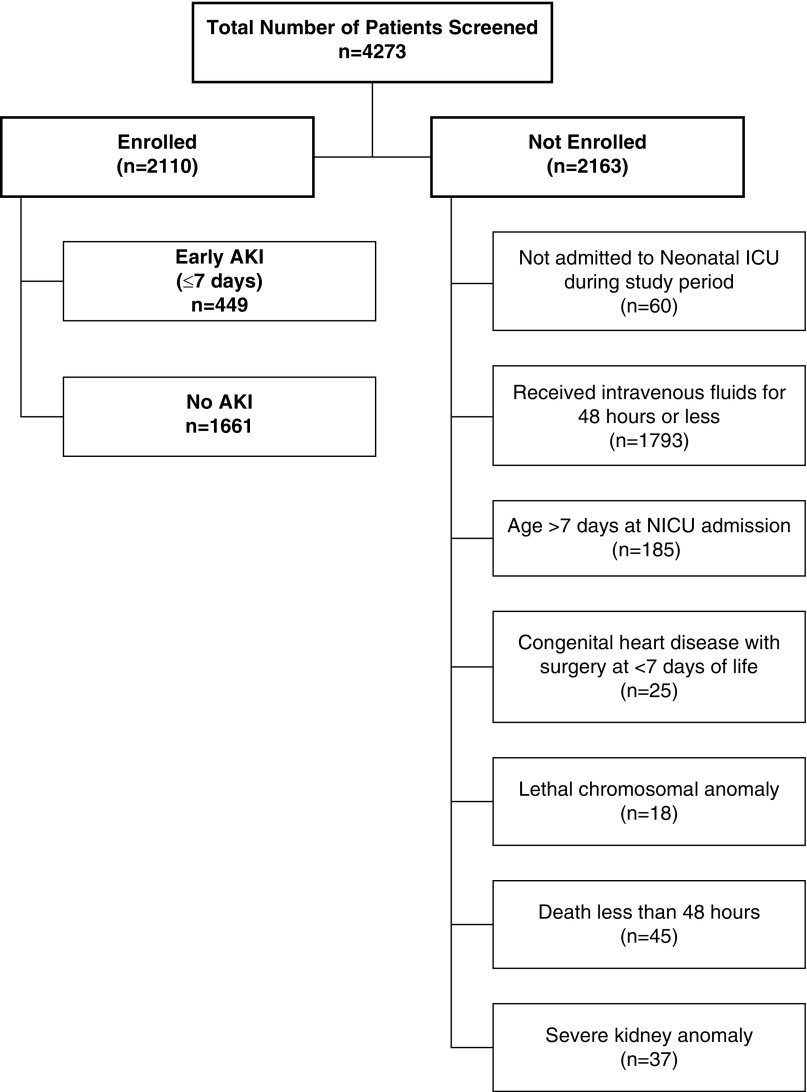
Design, setting, participants, & measurements: The international retrospective observational cohort study, Assessment of Worldwide AKI Epidemiology in Neonates (AWAKEN), included neonates admitted to a neonatal intensive care unit who received at least 48 hours of intravenous fluids. Early AKI was defined by an increase in serum creatinine >0.3 mg/dl or urine output <1 ml/kg per hour on postnatal days 2-7, the neonatal modification of Kidney Disease: Improving Global Outcomes criteria. We assessed risk factors for AKI and associations of AKI with death and duration of hospitalization.
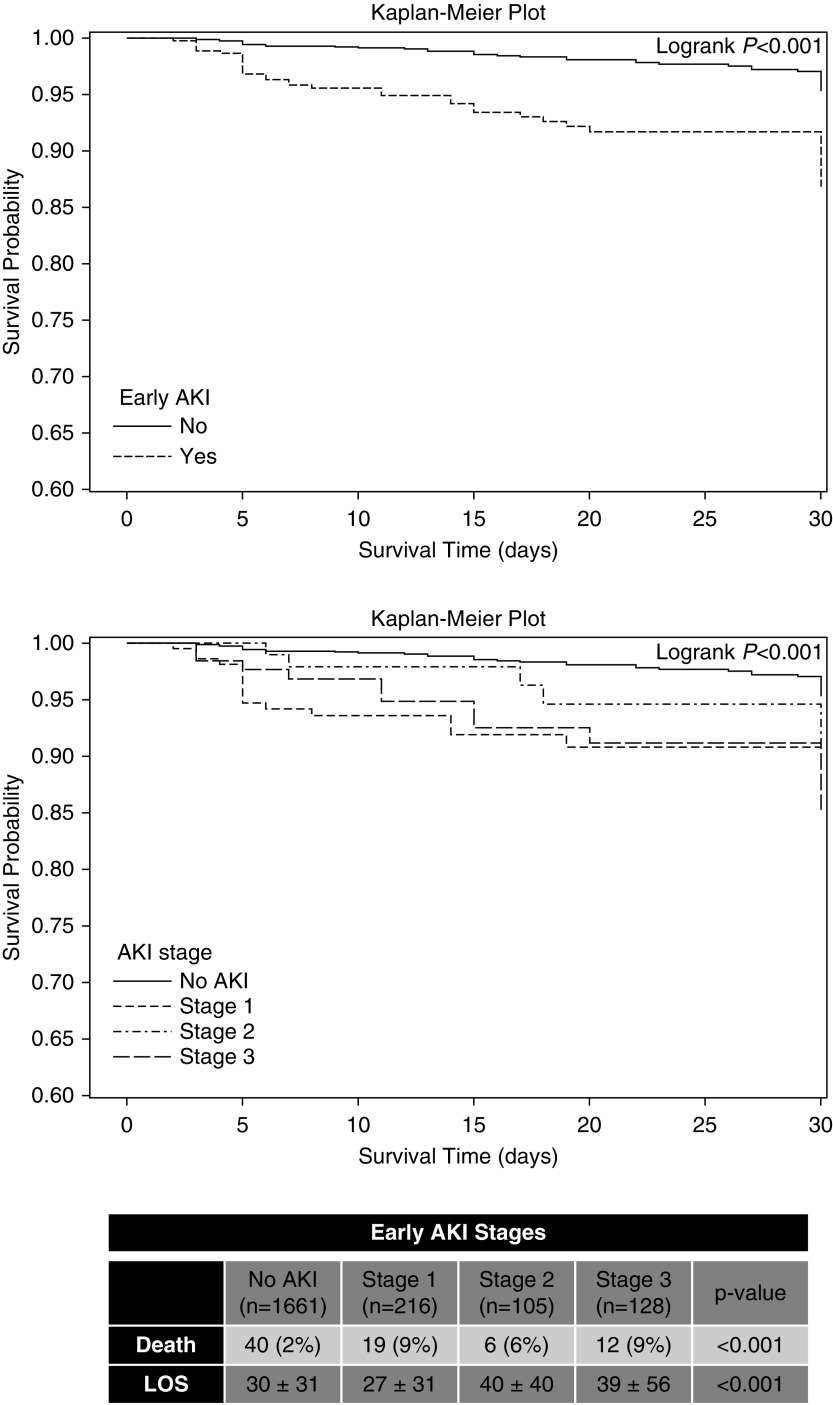
Results: Twenty-one percent (449 of 2110) experienced early AKI. Early AKI was associated with higher risk of death (adjusted odds ratio, 2.8; 95% confidence interval, 1.7 to 4.7) and longer duration of hospitalization (parameter estimate: 7.3 days 95% confidence interval, 4.7 to 10.0), adjusting for neonatal and maternal factors along with medication exposures. Factors associated with a higher risk of AKI included: outborn delivery; resuscitation with epinephrine; admission diagnosis of hyperbilirubinemia, inborn errors of metabolism, or surgical need; frequent kidney function surveillance; and admission to a children's hospital. Those factors that were associated with a lower risk included multiple gestations, cesarean section, and exposures to antimicrobials, methylxanthines, diuretics, and vasopressors. Risk factors varied by gestational age strata.
Conclusions: AKI in the first postnatal week is common and associated with death and longer duration of hospitalization. The AWAKEN study demonstrates a number of specific risk factors that should serve as "red flags" for clinicians at the initiation of the neonatal intensive care unit course.
Trial registration: ClinicalTrials.gov NCT02443389.
Keywords: Acute Kidney Injury; Anti-Infective Agents; Cesarean Section; Children; Epinephrine; Gestational Age; Hyperbilirubinemia; Incidence; Infant; Intensive Care Units; Mating Factor; Neonatal; Newborn; Pregnancy; Retrospective Studies; Vasoconstrictor Agents; Xanthines; child; creatinine; diuretics; hospitalization; methylxanthine; neonatal kidney collaborative; risk factors.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
- 172–174 doi: 10.2215/CJN.13461118
References
-
- Gadepalli SK, Selewski DT, Drongowski RA, Mychaliska GB: Acute kidney injury in congenital diaphragmatic hernia requiring extracorporeal life support: An insidious problem. J Pediatr Surg 46: 630–635, 2011 - PubMed
-
- Kaur S, Jain S, Saha A, Chawla D, Parmar VR, Basu S, Kaur J: Evaluation of glomerular and tubular renal function in neonates with birth asphyxia. Ann Trop Paediatr 31: 129–134, 2011 - PubMed
-
- Koralkar R, Ambalavanan N, Levitan EB, McGwin G, Goldstein S, Askenazi D: Acute kidney injury reduces survival in very low birth weight infants. Pediatr Res 69: 354–358, 2011 - PubMed
-
- Sarkar S, Askenazi DJ, Jordan BK, Bhagat I, Bapuraj JR, Dechert RE, Selewski DT: Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia. Pediatr Res 75: 431–435, 2014 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
