

Association of Premature Natural and Surgical Menopause With Incident Cardiovascular Disease
- PMID: 31738818
- PMCID: PMC7231649
- DOI: 10.1001/jama.2019.19191
Association of Premature Natural and Surgical Menopause With Incident Cardiovascular Disease
Abstract
Importance: Recent guidelines endorse using history of menopause before age 40 years to refine atherosclerotic cardiovascular disease risk assessments among middle-aged women. Robust data on cardiovascular disease risk in this population are lacking.
Objective: To examine the development of cardiovascular diseases and cardiovascular risk factors in women with natural and surgical menopause before age 40 years.
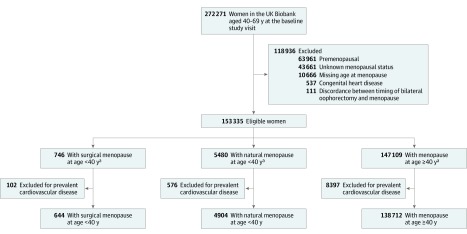
Design, setting, and participants: Cohort study (UK Biobank), with adult residents of the United Kingdom recruited between 2006 and 2010. Of women who were 40 to 69 years old and postmenopausal at study enrollment, 144 260 were eligible for inclusion. Follow-up occurred through August 2016.
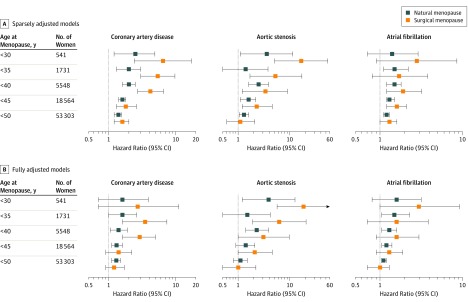
Exposures: Natural premature menopause (menopause before age 40 without oophorectomy) and surgical premature menopause (bilateral oophorectomy before age 40). Postmenopausal women without premature menopause served as the reference group.
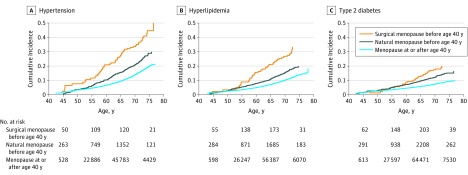
Main outcomes and measures: The primary outcome was a composite of incident coronary artery disease, heart failure, aortic stenosis, mitral regurgitation, atrial fibrillation, ischemic stroke, peripheral artery disease, and venous thromboembolism. Secondary outcomes included individual components of the primary outcome, incident hypertension, hyperlipidemia, and type 2 diabetes.
Results: Of 144 260 postmenopausal women included (mean [SD] age at enrollment, 59.9 [5.4] years), 4904 (3.4%) had natural premature menopause and 644 (0.4%) had surgical premature menopause. Participants were followed up for a median of 7 years (interquartile range, 6.3-7.7). The primary outcome occurred in 5415 women (3.9%) with no premature menopause (incidence, 5.70/1000 woman-years), 292 women (6.0%) with natural premature menopause (incidence, 8.78/1000 woman-years) (difference vs no premature menopause, +3.08/1000 woman-years [95% CI, 2.06-4.10]; P < .001), and 49 women (7.6%) with surgical premature menopause (incidence, 11.27/1000 woman-years) (difference vs no premature menopause, +5.57/1000 woman-years [95% CI, 2.41-8.73]; P < .001). For the primary outcome, natural and surgical premature menopause were associated with hazard ratios of 1.36 (95% CI, 1.19-1.56; P < .001) and 1.87 (95% CI, 1.36-2.58; P < .001), respectively, after adjustment for conventional cardiovascular disease risk factors and use of menopausal hormone therapy.
Conclusions and relevance: Natural and surgical premature menopause (before age 40 years) were associated with a small but statistically significant increased risk for a composite of cardiovascular diseases among postmenopausal women. Further research is needed to understand the mechanisms underlying these associations.
Conflict of interest statement
Figures
Comment in
-
Premature Menopause and Risk for Cardiovascular Disease.JAMA. 2020 Apr 28;323(16):1616-1617. doi: 10.1001/jama.2020.2530. JAMA. 2020. PMID: 32343322 No abstract available.
-
Premature Menopause and Risk for Cardiovascular Disease.JAMA. 2020 Apr 28;323(16):1616. doi: 10.1001/jama.2020.2533. JAMA. 2020. PMID: 32343323 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. ; Writing Group Members; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Heart disease and stroke statistics 2016 update: a report from the American Heart Association. Circulation. 2016;133(4):2411-2421. doi:10.1161/CIR.0000000000000350 - DOI - PubMed
