

Refined Sphenopalatine Ganglion Stimulator Placement and Intensity Setting to Augment Blood Flow and Neurologic Function
- PMID: 31739771
- PMCID: PMC7597988
- DOI: 10.1161/STROKEAHA.119.027177
Refined Sphenopalatine Ganglion Stimulator Placement and Intensity Setting to Augment Blood Flow and Neurologic Function
Abstract
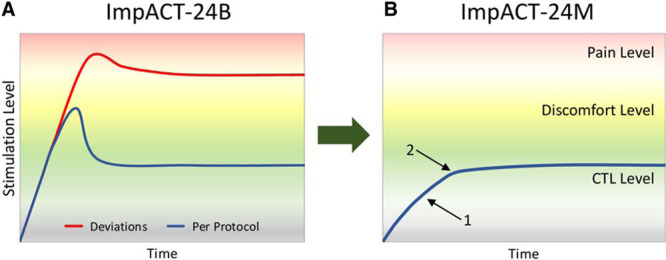
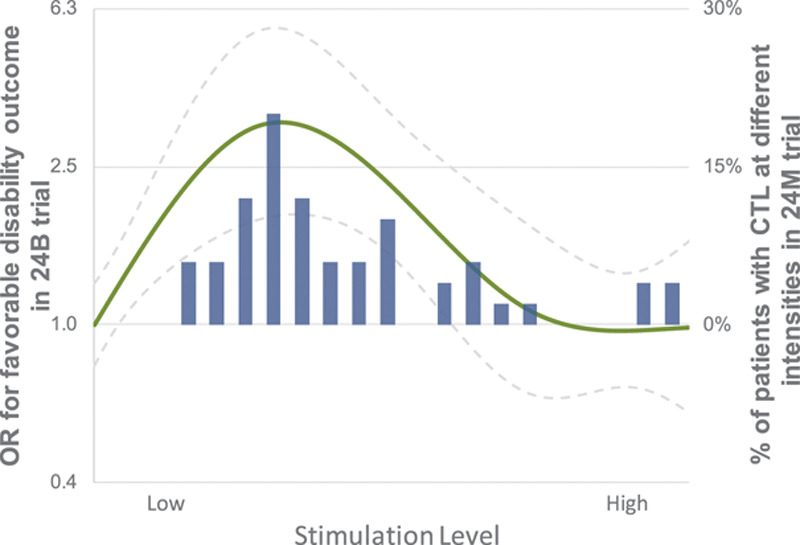
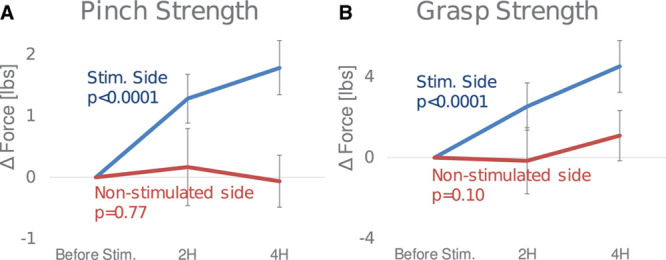
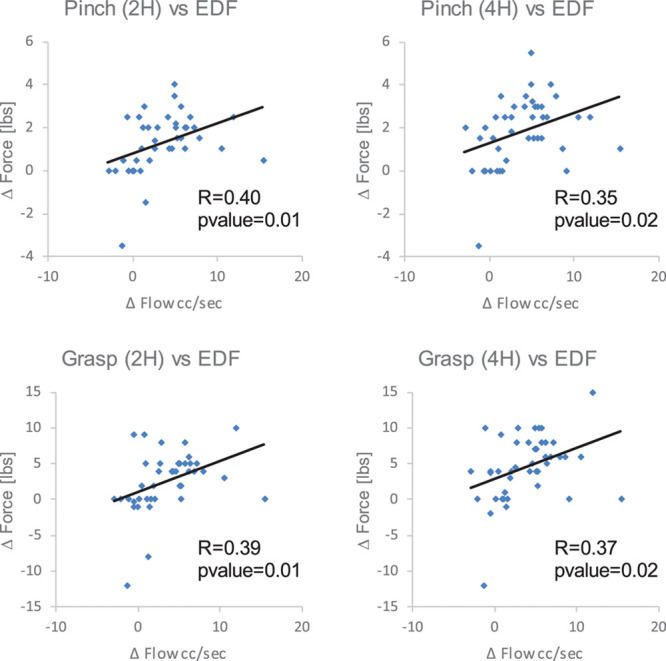
Background and Purpose- Two large, randomized trials indicated that sphenopalatine ganglion (SPG) stimulation improves final disability outcome in acute anterior circulation patients with ischemic stroke with confirmed cortical involvement. This study evaluated 2 refinements in SPG stimulation treatment technique: (1) SPG electrode placement with real-time optical tracking guidance; and (2) stimulation intensity comfortable tolerance level selection using non-noxious facial physiological markers. Methods- This study was a single, active arm trial at 4 centers, enrolling patients with anterior circulation ischemic stroke, National Institutes of Health Stroke Scale 1 to 6 including arm weakness subitem score ≥1, not receiving recanalization therapies, and within 24 hours of onset. Stimulation level was set based on ipsilateral facial tingling sensation or lacrimation. SPG stimulation effects were assessed by measuring volumetric blood flow in the ipsilateral common carotid artery by ultrasound and grasp and pinch strength in the affected hand before and during stimulation, and by change in National Institutes of Health Stroke Scale from day 1 to 7. Results- Among 50 enrolled patients, age was median 66 years (interquartile range, 60-74), 44% were female, National Institutes of Health Stroke Scale median was 5 (interquartile range, 4-5), and median onset-to-screening time was 18 hours (interquartile range, 9-20). Median implantation skin-to-skin time was 4 minutes (interquartile range, 3-7), and all 50 implants were placed correctly. Comfortable tolerance level was found based on physiological biomarkers in 96% of patients, including 86% in the optimal, low-medium intensity range. SPG stimulation significantly increased common carotid artery peak systolic and end-diastolic blood flow (44%, P<0.0001; and 52%, P<0.0001) and improved pinch strength (42%, P<0.0001) and grasp strength (26%, P<0.0001). Degree of National Institutes of Health Stroke Scale recovery by day 7 was greater than in matched historic controls, median 75% versus 50%, P=0.0003. Conclusions- SPG stimulator placement with real-time optical tracking guidance was fast and accurate, and selection of stimulation intensity levels based on non-noxious facial tingling and lacrimation was feasible in nearly all patients. SPG stimulation led to cervico-cranial blood flow augmentation and improved hand motor function. Clinical Trial Registration- URL: https://www.clinicaltrials.gov. Unique identifier: NCT03551093.
Keywords: biomarker; collateral circulation; electrode; ganglia; hand strength; nasolacrimal duct; pinch strength.
Figures
References
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Menash GE, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob Health. 2013;1:e259–e281. doi: 10.1016/S2214-109X(13)70089-5. - PMC - PubMed
-
- Turc G, Bhogal P, Fischer U, Khatri P, Lobotesis K, Mazighi M, et al. European Stroke Organisation (ESO)- European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2019;11:535–538. doi: 10.1136/neurintsurg-2018-014568. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. American Heart Association Stroke Council. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–e110. doi: 10.1161/STR.0000000000000158. - PubMed
-
- Rai AT, Seldon AE, Boo S, Link PS, Domico JR, Tarabishy AR, et al. A population-based incidence of acute large vessel occlusions and thrombectomy eligible patients indicates significant potential for growth of endovascular stroke therapy in the USA. J Neurointerv Surg. 2017;9:722–726. doi: 10.1136/neurintsurg-2016-012515. - PMC - PubMed
-
- Shuaib A, Butcher K, Mohammad AA, Saqqur M, Liebeskind DS. Collateral blood vessels in acute ischaemic stroke: a potential therapeutic target. Lancet Neurol. 2011;10:909–921. doi: 10.1016/S1474-4422(11)70195-8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
