

Long-Term Objective Adherence to Mandibular Advancement Device Therapy Versus Continuous Positive Airway Pressure in Patients With Moderate Obstructive Sleep Apnea
- PMID: 31739856
- PMCID: PMC6853388
- DOI: 10.5664/jcsm.8034
Long-Term Objective Adherence to Mandibular Advancement Device Therapy Versus Continuous Positive Airway Pressure in Patients With Moderate Obstructive Sleep Apnea
Abstract
Study objectives: Comparable health effects of mandibular advancement device (MAD) and continuous positive airway pressure (CPAP) therapy have been attributed to higher adherence with MAD compared with CPAP therapy. The objective of this study was to make a direct comparison of the objective adherence between MAD and CPAP in patients with moderate obstructive sleep apnea (OSA).
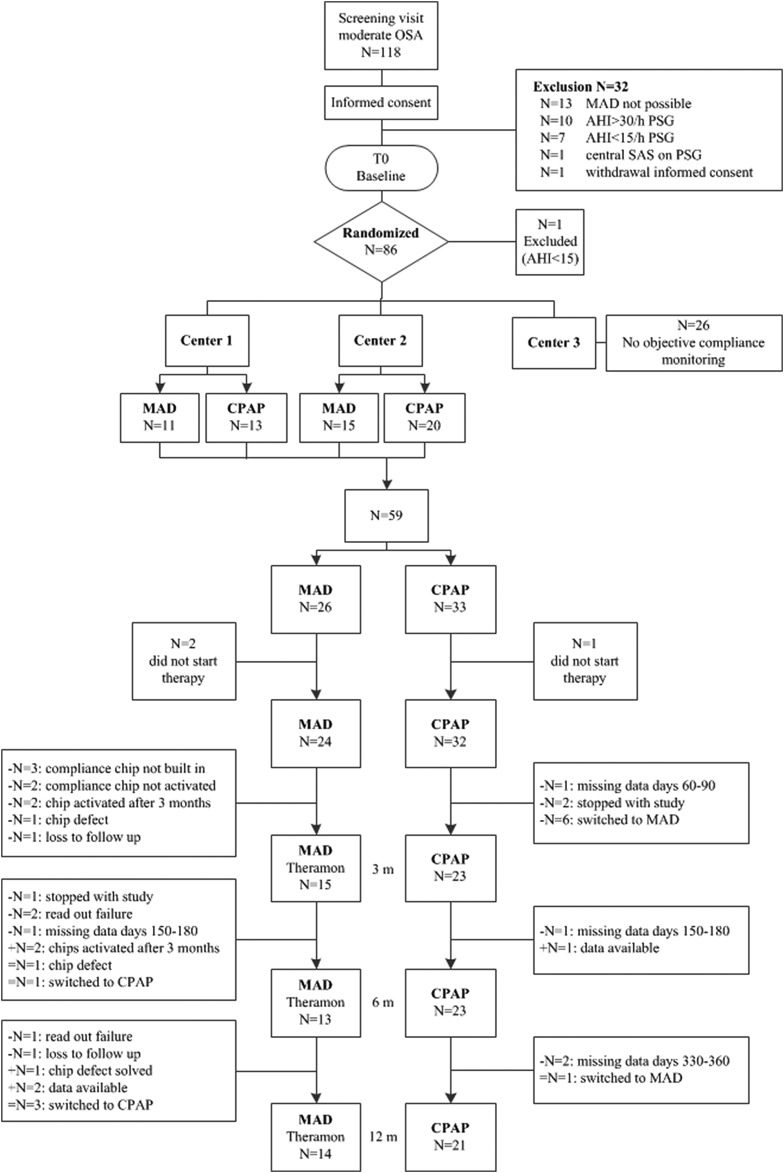
Methods: Adherence was monitored for 12 months in 59 patients with moderate OSA (apnea-hypopnea index 15-30 events/h) as part of a randomized controlled trial. Objective adherence with MAD was assessed using the TheraMon microsensor. Objective adherence with CPAP was assessed using the built-in registration software with readout on SD card. Self-reported adherence with both therapies was assessed using a questionnaire.
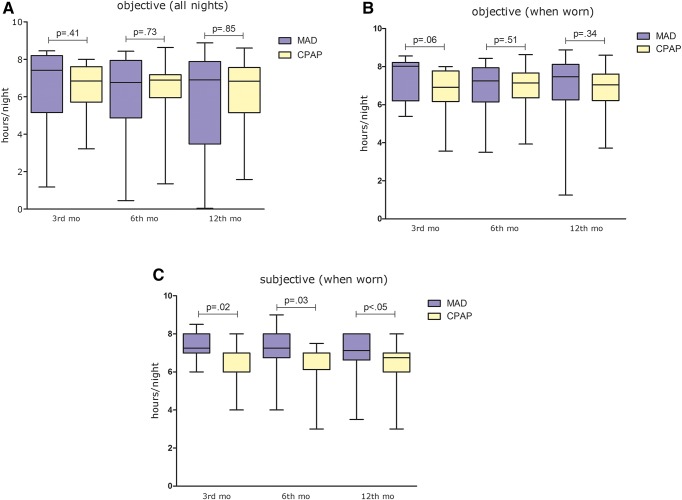
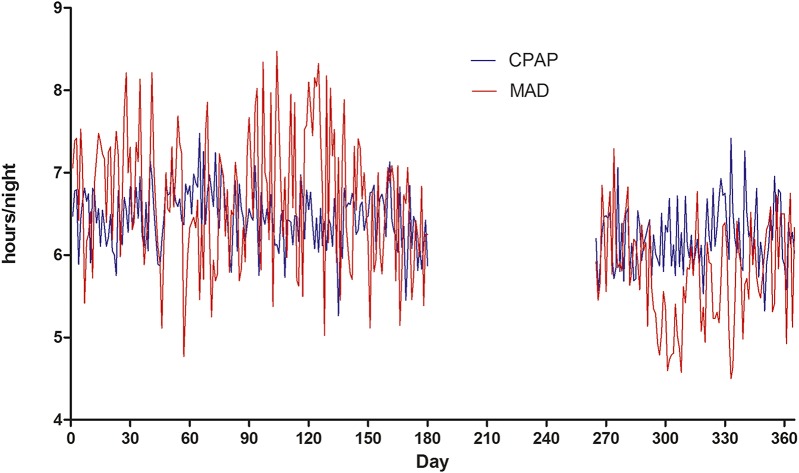
Results: Forty patients (68%) completed the study with the therapy to which they were randomly assigned. Median (interquartile range) objective adherence (h/night) in the 3rd month was 7.4 (5.2-8.2) for MAD and 6.8 (5.7-7.6) for CPAP (P = .41), compared to 6.9 (3.5-7.9) with MAD and 6.8 (5.2-7.6) with CPAP (P = .85) in the 12th month. There were no significant changes between the 3rd and 12th month for both MAD (P = .21) and CPAP (P = .46). Changes in adherence were not significantly different between MAD and CPAP (P = .51). Self-reported adherence was significantly higher with MAD than CPAP at all follow-ups. Self-reported adherence with CPAP was lower than objective CPAP adherence at the 6th and 12th month (P = .02).
Conclusions: Objective adherence with MAD and CPAP is comparable and consistent over time. Self-reported adherence is higher with MAD than with CPAP giving rise to interesting discrepancy between objective and self-reported adherence with CPAP.
Clinical trial registration: Registry: ClinicalTrials.gov; Identifier: NCT01588275.
Keywords: patient adherence; randomized controlled trial; sleep apnea.
© 2019 American Academy of Sleep Medicine.
Figures
References
-
- Lindberg E, Carter N, Gislason T, Janson C. Role of snoring and daytime sleepiness in occupational accidents. Am J Respir Crit Care Med. 2001;164(11):2031–2035. - PubMed
-
- Sjösten N, Kivimaki M, Oksanen T, et al. Obstructive sleep apnoea syndrome as a predictor of work disability. Respir Med. 2009;103(7):1047–1055. - PubMed
-
- Rodenstein D. Sleep apnea: traffic and occupational accidents–individual risks, socioeconomic and legal implications. Respiration. 2009;78(3):241–248. - PubMed
-
- Terán-Santos J, Jimenez-Gomez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. cooperative group burgos-santander. N Engl J Med. 1999;340(11):847–851. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
