

Association of maternal antiretroviral use with microcephaly in children who are HIV-exposed but uninfected (SMARTT): a prospective cohort study
- PMID: 31740351
- PMCID: PMC6952580
- DOI: 10.1016/S2352-3018(19)30340-6
Association of maternal antiretroviral use with microcephaly in children who are HIV-exposed but uninfected (SMARTT): a prospective cohort study
Abstract
Background: Perinatal HIV transmission has substantially decreased with combination antiretroviral regimens, but complications in children who are HIV-exposed but uninfected, such as microcephaly, warrant ongoing surveillance. We aimed to evaluate whether individual in utero antiretroviral exposures were associated with increased risk of microcephaly based on long-term follow-up of infants and children who are HIV-exposed but uninfected.
Methods: We evaluated children aged younger than 18 years who were HIV-exposed but uninfected with at least one head circumference measurement while enrolled in the Surveillance Monitoring for ART Toxicities (SMARTT) study at 22 clinical sites in the USA, including Puerto Rico. This prospective cohort study was done by the Pediatric HIV/AIDS Cohort Study network. Microcephaly was defined as having a head circumference Z score <-2 according to the 2000 US Centers for Disease Control and Prevention growth charts for children 6-36 months old and according to Nellhaus standards (head circumference <2nd percentile) after 36 months (SMARTT criteria); an alternate definition for microcephaly was based on applying Nellhaus standards across all ages (Nellhaus criteria). Modified Poisson regression models were fit to obtain relative risks (RRs) for associations between in utero antiretroviral exposure and microcephaly status, adjusted for potential confounders. Neurodevelopmental functioning was compared in children who are HIV-exposed but uninfected with or without microcephaly.
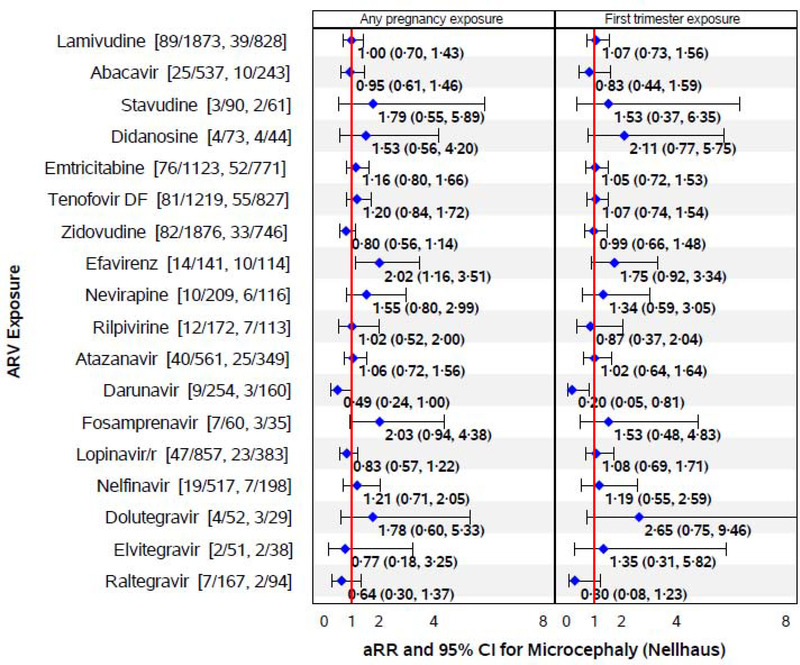
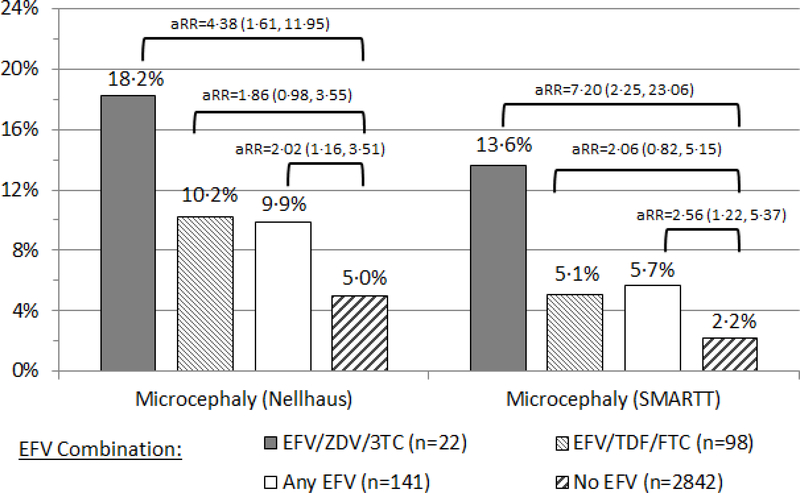
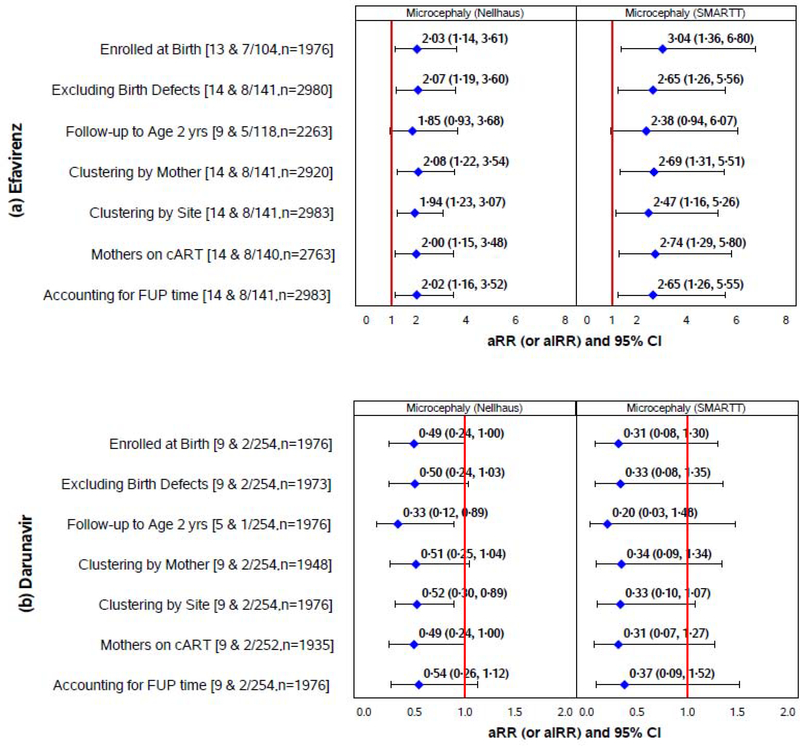
Findings: Between March 21, 2007, and Aug 1, 2017, 3055 participants enrolled in SMARTT had at least one head circumference measurement. The cumulative incidence of microcephaly over a median of 5·1 years of follow-up (IQR 3·0-7·2) was 159 (5·2%, 95% CI 4·4-6·1) by Nellhaus criteria and 70 (2·3%, 1·8-2·9) by SMARTT criteria. In adjusted models, in utero exposure to efavirenz (4·7% exposed) was associated with increased risk of microcephaly by both Nellhaus standards (adjusted RR 2·02, 95% CI 1·16-3·51) and SMARTT criteria (2·56, 1·22-5·37). These associations were more pronounced in children exposed to combination regimens of efavirenz that included zidovudine plus lamivudine than those including tenofovir plus emtricitabine. Protective associations were observed for darunavir exposure (adjusted RR 0·50, 95% CI 0·24-1·00). Children who are HIV-exposed but uninfected with microcephaly had lower mean scores on neurodevelopmental assessments at age 1 and 5 years and a higher prevalence of neurodevelopmental impairment than those without microcephaly.
Interpretation: These findings support consideration of alternatives to efavirenz as part of first-line antiretroviral therapy for pregnant women.
Funding: Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Efavirenz in pregnancy.Lancet HIV. 2020 Jan;7(1):e6-e8. doi: 10.1016/S2352-3018(19)30330-3. Epub 2019 Nov 15. Lancet HIV. 2020. PMID: 31740349 No abstract available.
References
-
- Cooper ER, Charurat M, Mofenson L, Hanson IC, Pitt J, Diaz D, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1 infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2005; 29(5):484–494. - PubMed
-
- World Health Organization. Updated Recommendations on First-Line and Second-Line Antiretroviral Regimens and Post-Exposure Prophylaxis and Recommendations on Early Infant Diagnosis of HIV. Geneva, Switzerland: WHO; 2018. https://www.who.int/hiv/pub/guidelines/ARV2018update/en/, Accessed 5/2/2019.
-
- Rollins JD, Collins JS, Holden KR. United States head circumference growth reference charts: birth to 21 years. J Pediatr 2010; 156: 907–913. - PubMed
-
- Epstein LG, Gelbard HA. HIV-induced neuronal injury in the developing brain. J Leukoc Biol. 1999; 65:453–457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
