

Borderline Estrogen Receptor-Positive Breast Cancers in Black and White Women
- PMID: 31742342
- PMCID: PMC7357313
- DOI: 10.1093/jnci/djz206
Borderline Estrogen Receptor-Positive Breast Cancers in Black and White Women
Abstract
Background: Some breast tumors expressing greater than 1% and less than 10% estrogen receptor (ER) positivity (ER-borderline) are clinically aggressive; others exhibit luminal biology. Prior ER-borderline studies included few black participants.
Methods: Using the Carolina Breast Cancer Study (phase I: 1993-1996; 2: 1996-2001; 3: 2008-2013), a population-based study that oversampled black women, we compared ER-borderline (n = 217) to ER-positive (n = 1885) and ER-negative (n = 757) tumors. PAM50 subtype and risk of recurrence score (ROR-PT, incorporates subtype, proliferation, tumor size) were measured. Relative frequency differences (RFD) were estimated using multivariable linear regression. Disease-free interval (DFI) was evaluated by ER category and endocrine therapy receipt, overall and by race, using Kaplan Meier and Cox models. Statistical tests were two-sided.
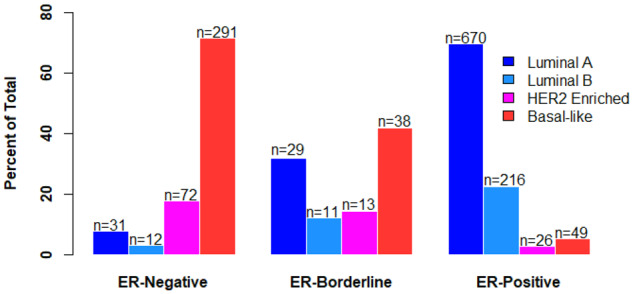
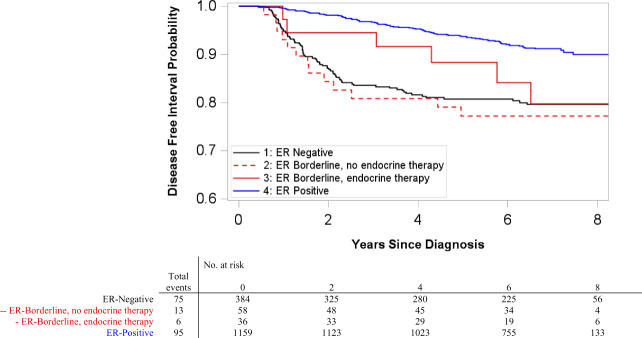
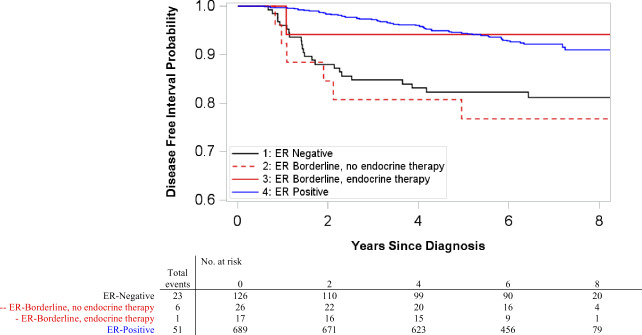
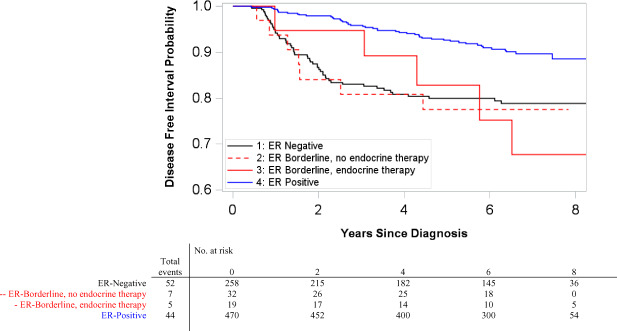
Results: ER-borderlines were more frequently basal-like (RFD = +37.7%, 95% confidence interval [CI] = 27.1% to 48.4%) and high ROR-PT (RFD = +52.4%, 95% CI = 36.8% to 68.0%) relative to ER-positives. Having a high ROR-PT ER-borderline tumor was statistically significantly associated with black race (RFD = +26.2%, 95% CI = 9.0% to 43.3%). Compared to ER-positives, DFI of ER-borderlines treated with endocrine therapy was poorer but not statistically significantly different (hazard ratio [HR] = 2.03, 95% CI = 0.89% to 4.65%), whereas DFI was statistically significantly worse for ER-borderlines without endocrine therapy (HR = 3.33, 95% CI = 1.84% to 6.02%). However, black women with ER-borderline had worse DFI compared to ER-positives, even when treated with endocrine therapy (HR = 2.77, 95% CI = 1.09% to 7.04%).
Conclusions: ER-borderline tumors were genomically heterogeneous, with survival outcomes that differed by endocrine therapy receipt and race. Black race predicted high-risk ER-borderlines and may be associated with poorer endocrine therapy response.
© The Author(s) 2019. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Elledge R, Allred D.. Clinical aspects of estrogen and progesterone receptors In: Diseases of the Breast. 3rd ed Philadelphia, PA: Lippincott Williams and Wilkins; 2004:602–617.
-
- Bartlett JM, Brookes CL, Robson T, et al. Estrogen receptor and progesterone receptor as predictive biomarkers of response to endocrine therapy: a prospectively powered pathology study in the Tamoxifen and Exemestane Adjuvant Multinational trial. J Clin Oncol. 2011;29(12):1531–1538. doi: 10.1200/JCO.2010.30.3677 - PMC - PubMed
-
- Harvey JM, Clark GM, Osborne CK, Allred DC.. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J Clin Oncol. 1999;17(5):1474–1481. - PubMed
-
- Pertschuk LP, Kim DS, Nayer K, et al. Immunocytochemical estrogen and progestin receptor assays in breast cancer with monoclonal antibodies. Histopathologic, demographic, and biochemical correlations and relationship to endocrine response and survival. Cancer. 1990;66(8):1663–1670. - PubMed
-
- Collins LC, Botero ML, Schnitt SJ.. Bimodal frequency distribution of estrogen receptor immunohistochemical staining results in breast cancer: an analysis of 825 cases. Am J Clin Pathol. 2005;123(1):16–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
