

Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients-A Randomized, Placebo-Controlled, Double-Blind Trial
- PMID: 31744243
- PMCID: PMC6912342
- DOI: 10.3390/jcm8112008
Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients-A Randomized, Placebo-Controlled, Double-Blind Trial
Abstract
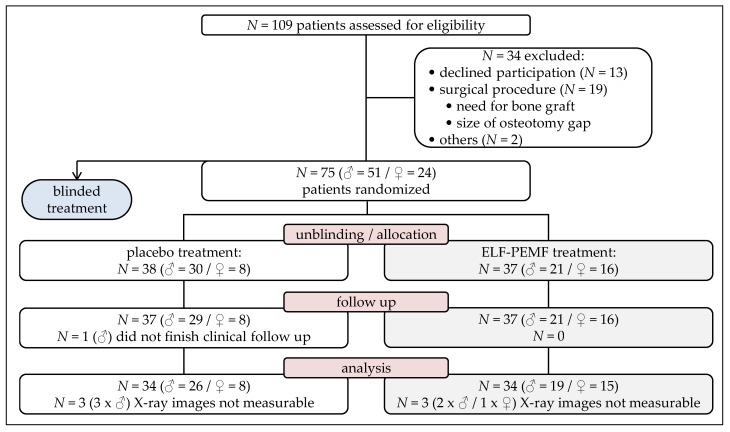
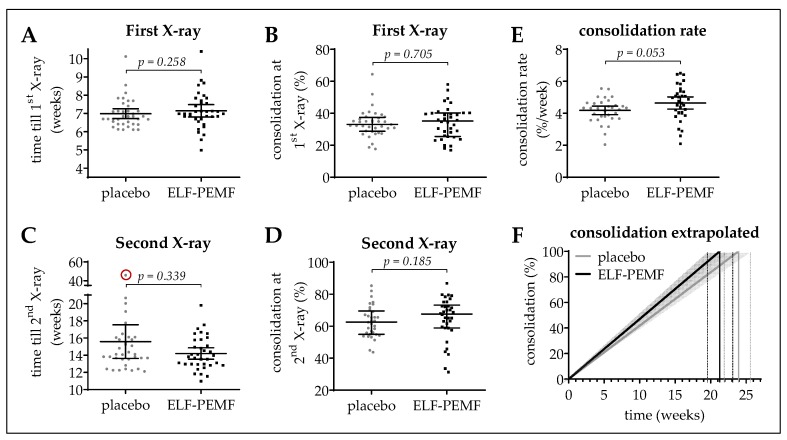
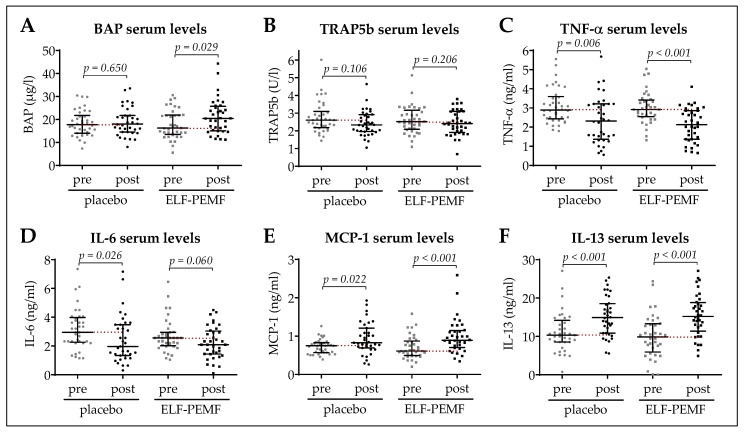
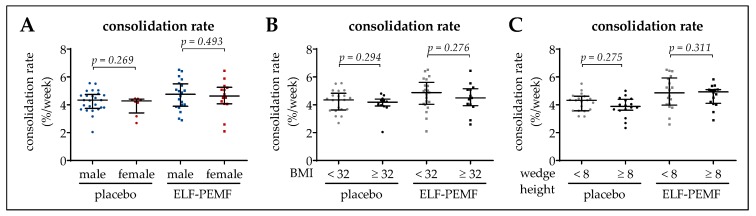
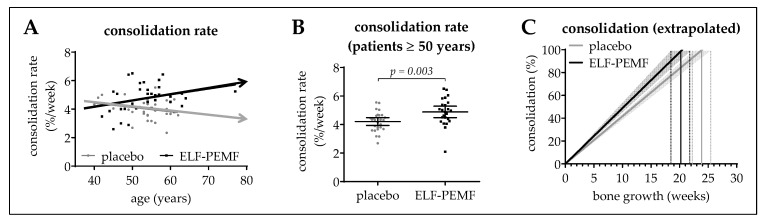
Extremely low-frequency pulsed electromagnetic field (ELF-PEMF) therapy is proposed to support bone healing after injuries and surgical procedures, being of special interest for elderly patients. This study aimed at investigating the effect of a specific ELF-PEMF, recently identified to support osteoblast function in vitro, on bone healing after high tibial osteotomy (HTO). Patients who underwent HTO were randomized to ELF-PEMF or placebo treatment, both applied by optically identical external devices 7 min per day for 30 days following surgery. Osseous consolidation was evaluated by post-surgical X-rays (7 and 14 weeks). Serum markers were quantified by ELISA. Data were compared by a two-sided t-test (α = 0.05). Device readouts showed excellent therapy compliance. Baseline parameters, including age, sex, body mass index, wedge height and blood cell count, were comparable between both groups. X-rays revealed faster osseous consolidation for ELF-PEMF compared to placebo treatment, which was significant in patients ≥50 years (∆mean = 0.68%/week; p = 0.003). Findings are supported by post-surgically increased bone-specific alkaline phosphatase serum levels following ELF-PEMF, compared to placebo (∆mean = 2.2 µg/L; p = 0.029) treatment. Adverse device effects were not reported. ELF-PEMF treatment showed a tendency to accelerate osseous consolidation after HTO. This effect was stronger and more significant for patients ≥50 years. This ELF-PEMF treatment might represent a promising adjunct to conventional therapy supporting osseous consolidation in elderly patients.
Keywords: bone specific alkaline phosphatase (BAP); elderly; extremely low frequency pulsed electromagnetic field (ELF-PEMF) therapy; high tibial osteotomy (HTO); osseous consolidation.
Conflict of interest statement
P.Z., A.K.N., B.W., F.S., A.Z., U.S., A.A., S.S., and S.E. declare no conflict of interest. K.F., A.-K.F., and G.E. are part of Sachtleben GmbH, manufacturer of the Somagen® device. K.F., A.-K.F., and G.E. were not involved in study design, collection, analyses or interpretation of data. A.Z. is scientific and statistical advisor to several companies working with electric medical devices or in the field of orthopedics, including Procon GmbH (Hamburg), Sachtleben GmbH (Hamburg) and Syntellix AG (Hannover).
Figures

References
-
- Massari L., Benazzo F., Falez F., Cadossi R., Perugia D., Pietrogrande L., Aloj D.C., Capone A., D’Arienzo M., Cadossi M., et al. Can clinical and surgical parameters be combined to predict how long it will take a tibia fracture to heal? A prospective multicentre observational study: The fracting study. Biomed. Res. Int. 2018;2018:1809091. doi: 10.1155/2018/1809091. - DOI - PMC - PubMed
-
- Massari L., Falez F., Lorusso V., Zanon G., Ciolli L., La Cava F., Cadossi M., Chiarello E., De Terlizzi F., Setti S., et al. Can a combination of different risk factors be correlated with leg fracture healing time? J. Orthop. Traumatol. 2013;14:51–57. doi: 10.1007/s10195-012-0218-7. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
