

Implementation of earlier antibiotic administration in patients with severe sepsis and septic shock in Japan: a descriptive analysis of a prospective observational study
- PMID: 31744549
- PMCID: PMC6862854
- DOI: 10.1186/s13054-019-2644-x
Implementation of earlier antibiotic administration in patients with severe sepsis and septic shock in Japan: a descriptive analysis of a prospective observational study
Abstract
Background: Time to antibiotic administration is a key element in sepsis care; however, it is difficult to implement sepsis care bundles. Additionally, sepsis is different from other emergent conditions including acute coronary syndrome, stroke, or trauma. We aimed to describe the association between time to antibiotic administration and outcomes in patients with severe sepsis and septic shock in Japan.
Methods: This prospective observational study enrolled 1184 adult patients diagnosed with severe sepsis based on the Sepsis-2 criteria and admitted to 59 intensive care units (ICUs) in Japan between January 1, 2016, and March 31, 2017, as the sepsis cohort of the Focused Outcomes Research in Emergency Care in Acute Respiratory Distress Syndrome, Sepsis and Trauma (FORECAST) study. We compared the characteristics and in-hospital mortality of patients administered with antibiotics at varying durations after sepsis recognition, i.e., 0-60, 61-120, 121-180, 181-240, 241-360, and 361-1440 min, and estimated the impact of antibiotic timing on risk-adjusted in-hospital mortality using the generalized estimating equation model (GEE) with an exchangeable, within-group correlation matrix, with "hospital" as the grouping variable.
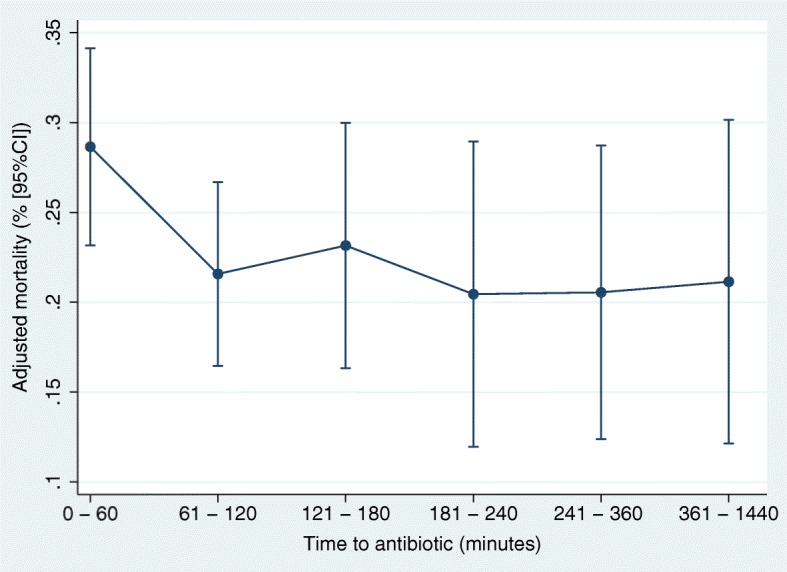
Results: Data from 1124 patients in 54 hospitals were used for analyses. Of these, 30.5% and 73.9% received antibiotics within 1 h and 3 h, respectively. Overall, the median time to antibiotic administration was 102 min [interquartile range (IQR), 55-189]. Compared with patients diagnosed in the emergency department [90 min (IQR, 48-164 min)], time to antibiotic administration was shortest in patients diagnosed in ICUs [60 min (39-180 min)] and longest in patients transferred from wards [120 min (62-226)]. Overall crude mortality was 23.4%, where patients in the 0-60 min group had the highest mortality (28.0%) and a risk-adjusted mortality rate [28.7% (95% CI 23.3-34.1%)], whereas those in the 61-120 min group had the lowest mortality (20.2%) and risk-adjusted mortality rates [21.6% (95% CI 16.5-26.6%)]. Differences in mortality were noted only between the 0-60 min and 61-120 min groups.
Conclusions: We could not find any association between earlier antibiotic administration and reduction in in-hospital mortality in patients with severe sepsis.
Keywords: Antibiotic; Bundle; Protocols; Sepsis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Implementation of earlier antibiotic administration in patients with severe sepsis and septic shock in Japan: antibiotic action needs time and tissue perfusion to reach target.Crit Care. 2020 Jan 14;24(1):17. doi: 10.1186/s13054-020-2727-8. Crit Care. 2020. PMID: 31937340 Free PMC article. No abstract available.
References
-
- Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign bundle: 2018 update. Intensive Care Med. 2018;46:997–1000. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
