

Musculoskeletal Pain, Physical Function, and Quality of Life After Bariatric Surgery
- PMID: 31744891
- PMCID: PMC6889948
- DOI: 10.1542/peds.2019-1399
Musculoskeletal Pain, Physical Function, and Quality of Life After Bariatric Surgery
Abstract
Objectives: To evaluate the longitudinal effects of metabolic and bariatric surgery (MBS) on the prevalence of musculoskeletal and lower extremity (LE) pain, physical function, and health-related quality of life.
Methods: The Teen Longitudinal Assessment of Bariatric Surgery study (NCT00474318) prospectively collected data on 242 adolescents undergoing MBS at 5 centers over a 3-year follow-up. Joint pain and physical function outcomes were assessed by using the Health Assessment Questionnaire Disability Index, Impact of Weight on Quality of Life - Kids, and the Short Form 36 Health Survey. Adolescents with Blount disease (n = 9) were excluded.
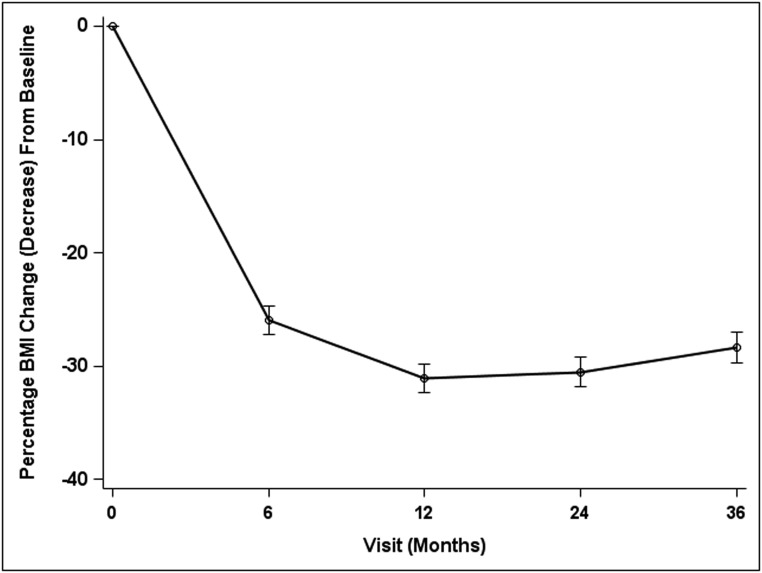
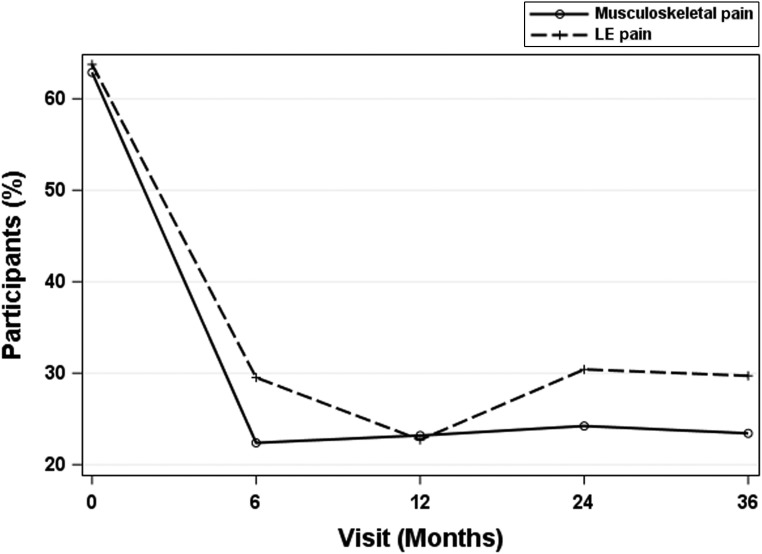
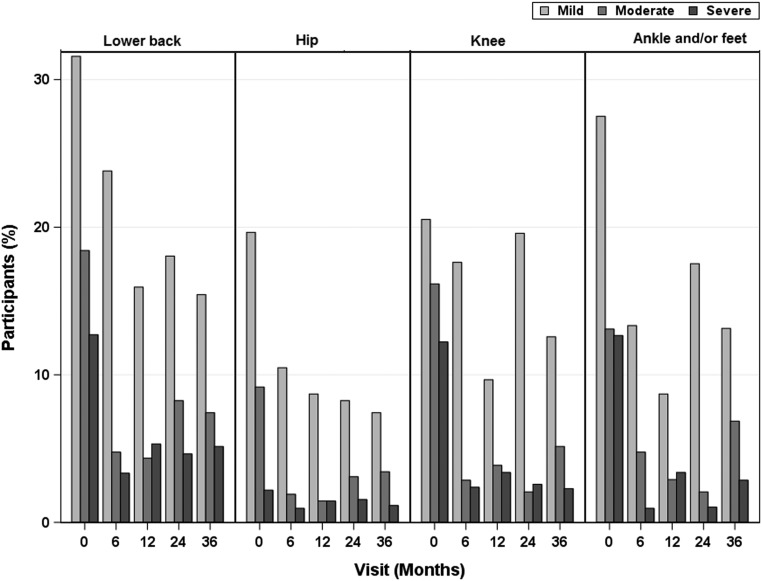
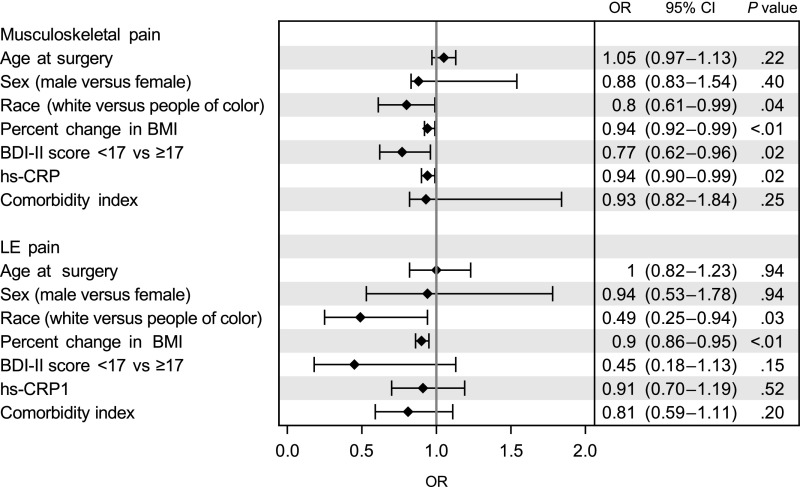
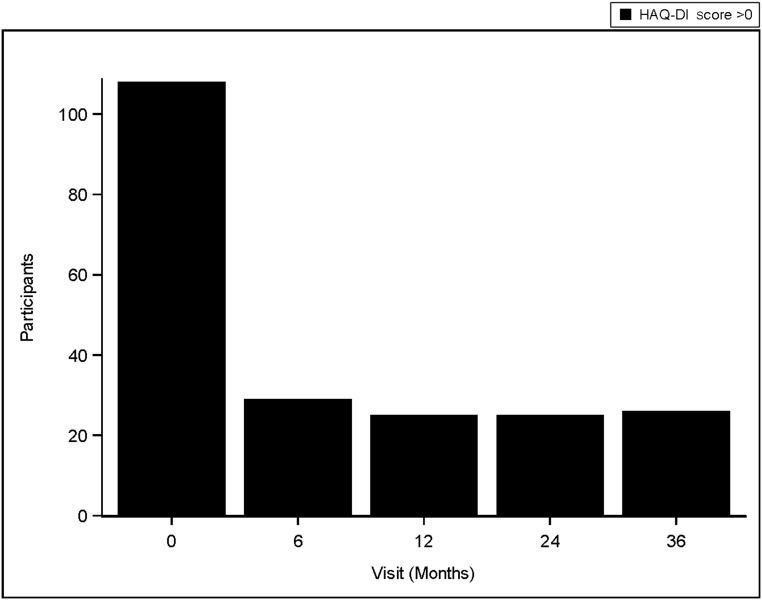
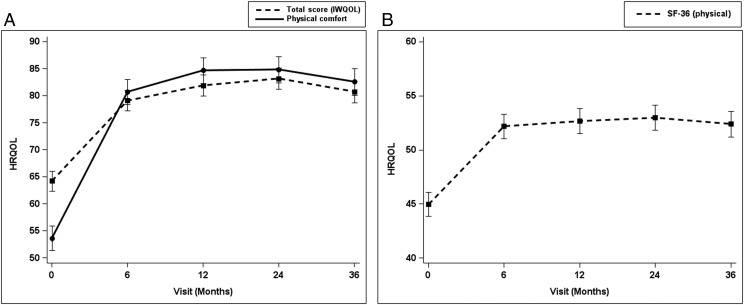
Results: Prevalent musculoskeletal and LE pain were reduced by 40% within 12 months and persisted over 3 years. Adjusted models revealed a 6% lower odds of having musculoskeletal pain (odds ratio = 0.94, 95% confidence interval: 0.92-0.99) and a 10% lower odds of having LE pain (odds ratio = 0.90, 95% confidence interval: 0.86-0.95) per 10% reduction of BMI. The prevalence of poor physical function (Health Assessment Questionnaire Disability Index score >0) declined from 49% to <20% at 6 months (P < .05), Physical comfort and the physical component scores, measured by the Impact of Weight on Quality of Life - Kids and the Short Form 36 Health Survey, improved at 6 months postsurgery and beyond (P < .01). Poor physical function predicted persistent joint pain after MBS.
Conclusions: Joint pain, impaired physical function, and impaired health-related quality of life significantly improve after MBS. These benefits in patient-reported outcomes support the use of MBS in adolescents with severe obesity and musculoskeletal pain and suggest that MBS in adolescence may reverse and reduce multiple risk factors for future joint disease.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: Dr Inge received honoraria and stock options from Standard Bariatrics and honoraria from UpToDate and Independent Medical Expert Consulting Services and served as a consultant for Zafgen, Inc, BioMedical Insights, and L&E Research, all outside the submitted work. Dr Harmon served on an advisory panel for Stryker Corporation from 1998 to 2015, unrelated to this project. Dr Dixon consulted for Apollo Endosurgery, Covidien, Bariatric Advantage, Nestle Health Science, Inova, and Novo Nordisk; the other authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Deere KC, Clinch J, Holliday K, et al. Obesity is a risk factor for musculoskeletal pain in adolescents: findings from a population-based cohort. Pain. 2012;153(9):1932–1938 - PubMed
-
- Gushue DL, Houck J, Lerner AL. Effects of childhood obesity on three-dimensional knee joint biomechanics during walking. J Pediatr Orthop. 2005;25(6):763–768 - PubMed
-
- Widhalm HK, Seemann R, Hamboeck M, et al. Osteoarthritis in morbidly obese children and adolescents, an age-matched controlled study. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):644–652 - PubMed
-
- Gelber AC, Hochberg MC, Mead LA, et al. Body mass index in young men and the risk of subsequent knee and hip osteoarthritis. Am J Med. 1999;107(6):542–548 - PubMed
