

Prediction and associations of preterm birth and its subtypes with eicosanoid enzymatic pathways and inflammatory markers
- PMID: 31745121
- PMCID: PMC6863859
- DOI: 10.1038/s41598-019-53448-z
Prediction and associations of preterm birth and its subtypes with eicosanoid enzymatic pathways and inflammatory markers
Abstract
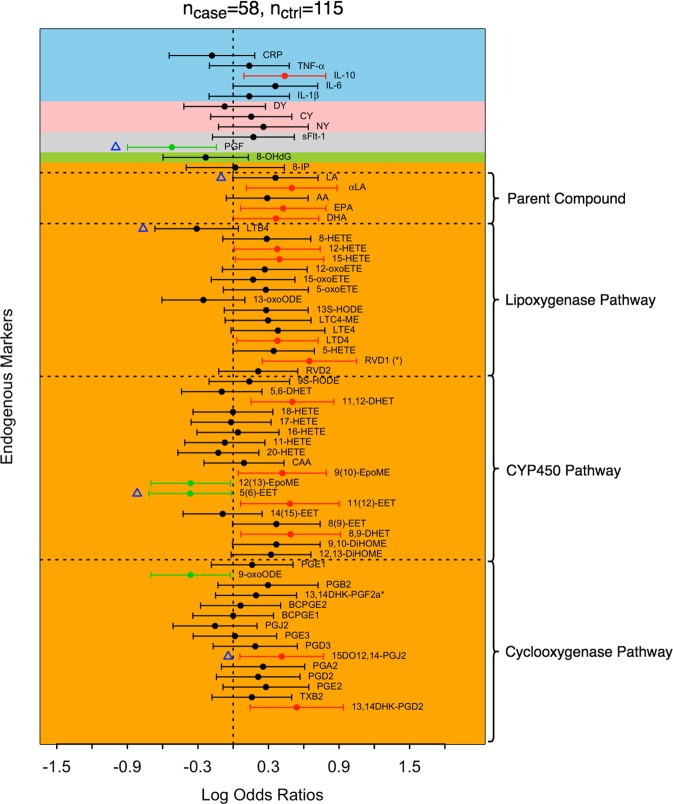
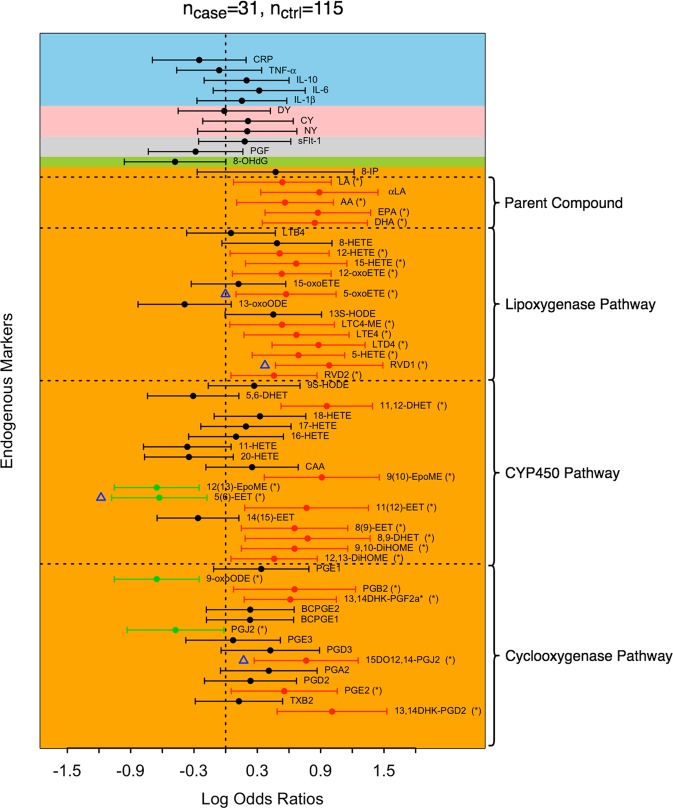
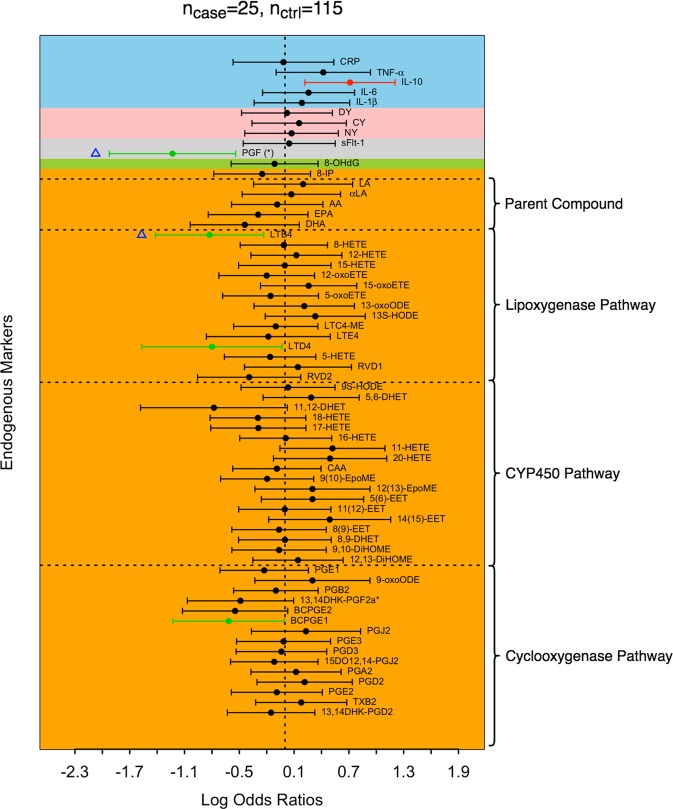
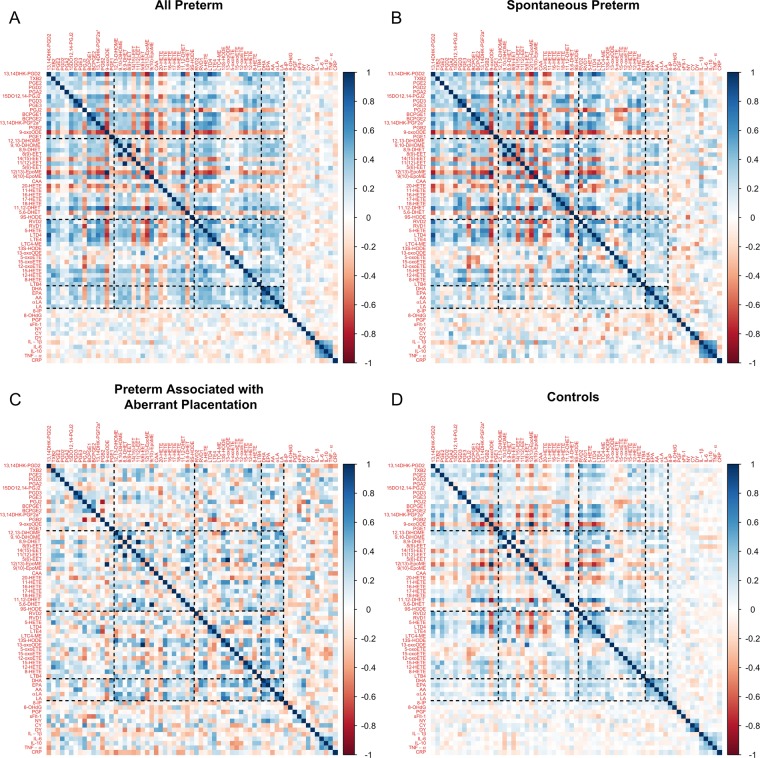
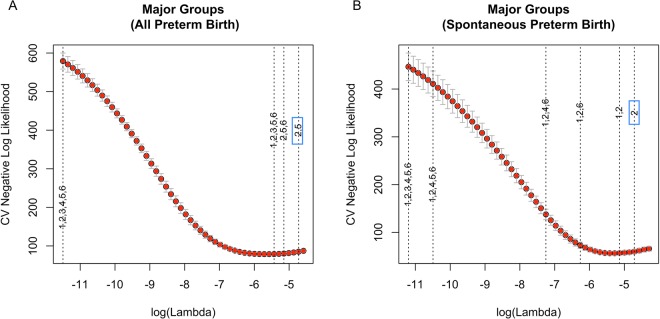
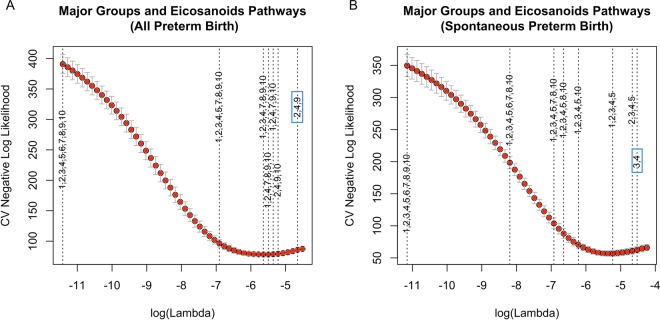
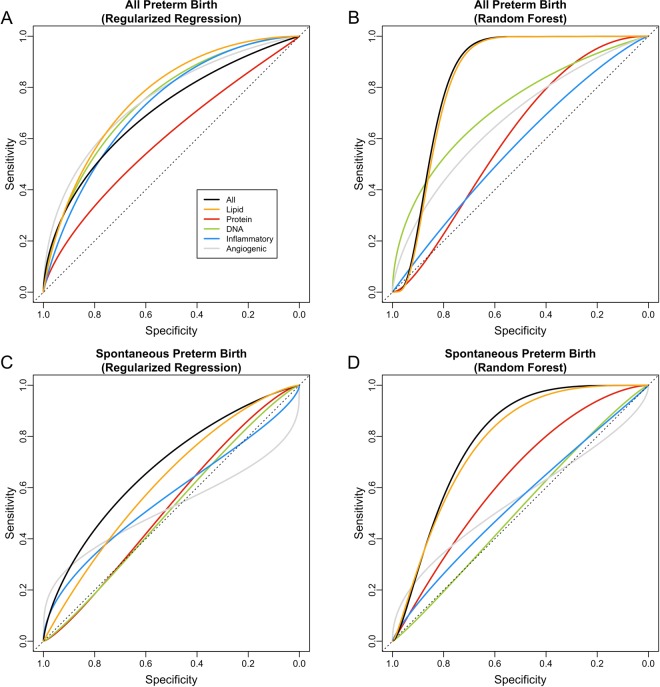
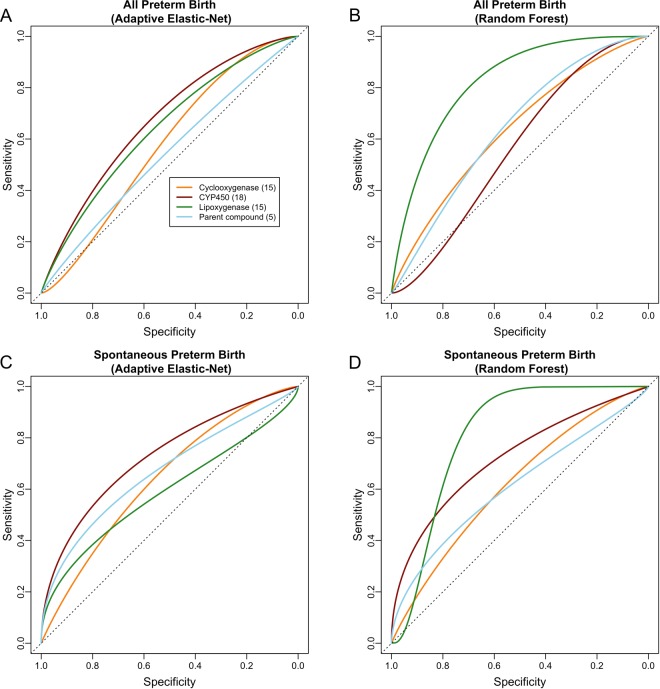
Endogenous signaling molecules derived from lipids, peptides, and DNA, are important regulators of physiological processes during pregnancy. The effect of their collective impact on preterm birth (delivery < 37 weeks gestation) is understudied. We aimed to characterize the associations and predictive capacity of an extensive panel of eicosanoids, immune biomarkers, oxidative stress markers, and growth factors towards preterm birth and its subtypes. We conducted a cross-sectional study of pregnant women (recruited < 15 weeks gestation) in the LIFECODES birth cohort, which included 58 cases of preterm birth and 115 controls that delivered term. Among the cases there were 31 cases who had a spontaneous preterm birth (cases who had spontaneous preterm labor and/or preterm premature rupture of membranes) and 25 that had preterm birth associated with aberrant placentation (cases who had preeclampsia and/or intrauterine growth restriction) and 2 cases that could not be sufficiently categorized as either. We analyzed single biomarker associations with each preterm birth outcome using multiple logistic regression. Adaptive elastic-net was implemented to perform a penalized multiple logistic regression on all biomarkers simultaneously to identify the most predictive biomarkers. We then organized biomarkers into biological groups and by enzymatic pathways and applied adaptive elastic-net and random forest to evaluate the accuracy of each group for predicting preterm birth cases. The majority of associations we observed were for spontaneous preterm birth, and adaptive elastic-net identified 5-oxoeicosatetraenoic acid, resolvin D1, 5,6-epoxy-eicsatrienoic acid, and 15-deoxy-12,14-prostaglandin J2 as most predictive. Overall, lipid biomarkers performed the best at separating cases from controls compared to other biomarker categories (adaptive elastic-net AUC = 0.78 [0.62, 0.94], random forest AUC = 0.84 [0.72, 0.96]). Among the enzymatic pathways that differentiate eicosanoid metabolites, we observed the highest prediction of overall preterm birth by lipoxygenase metabolites using random forest (AUC = 0.83 [0.69, 0.96]), followed by cytochrome p450 metabolites using adaptive elastic-net (AUC = 0.74 [0.52, 0.96]). In this study we translate biological hypothesis into the language of modern machine learning. Many lipid biomarkers were highly associated with overall and spontaneous preterm birth. Among eicosanoids, lipoxygenase and cytochrome p450 products performed best in identifying overall and spontaneous preterm birth. The combination of lipid biomarkers may have good utility in clinical settings to predict preterm birth.
Conflict of interest statement
The authors declare they have no competing financial or non-financial interests as defined by Nature Research, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures
References
-
- Institute of Medicine. Preterm Birth: Causes, Consequences, and Prevention, 10.17226/11622 (2007).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
