

Characteristics of Patent Ductus Arteriosus in Congenital Rubella Syndrome
- PMID: 31745134
- PMCID: PMC6863812
- DOI: 10.1038/s41598-019-52936-6
Characteristics of Patent Ductus Arteriosus in Congenital Rubella Syndrome
Abstract
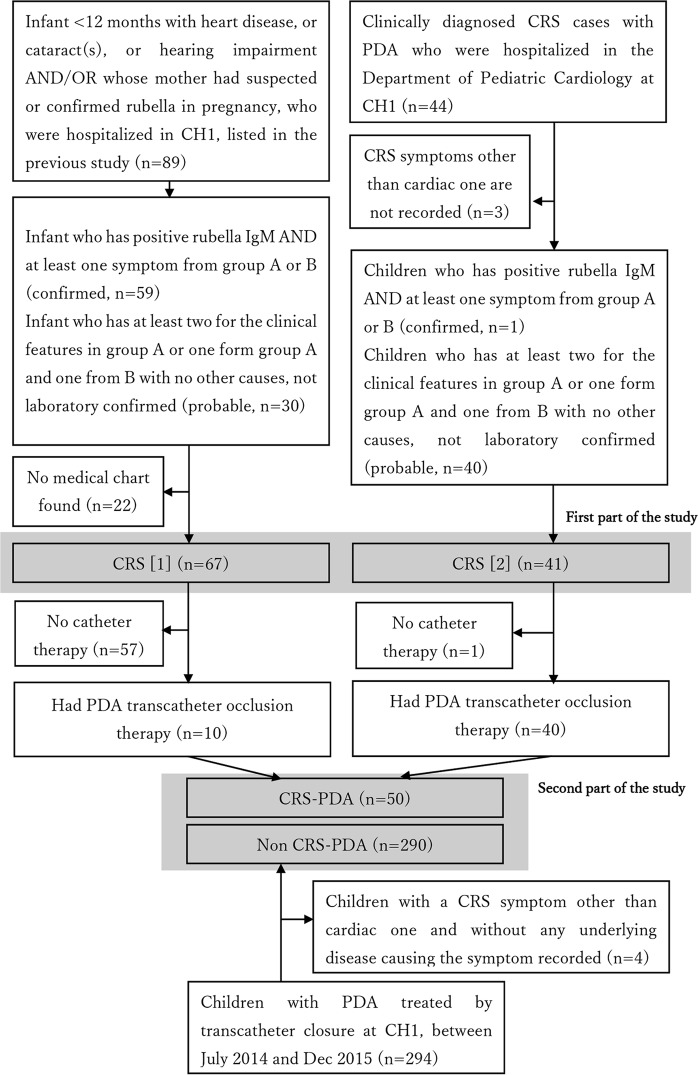
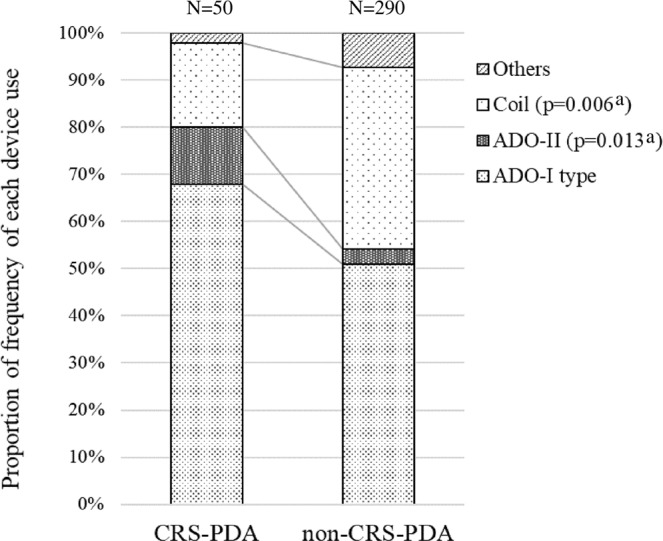
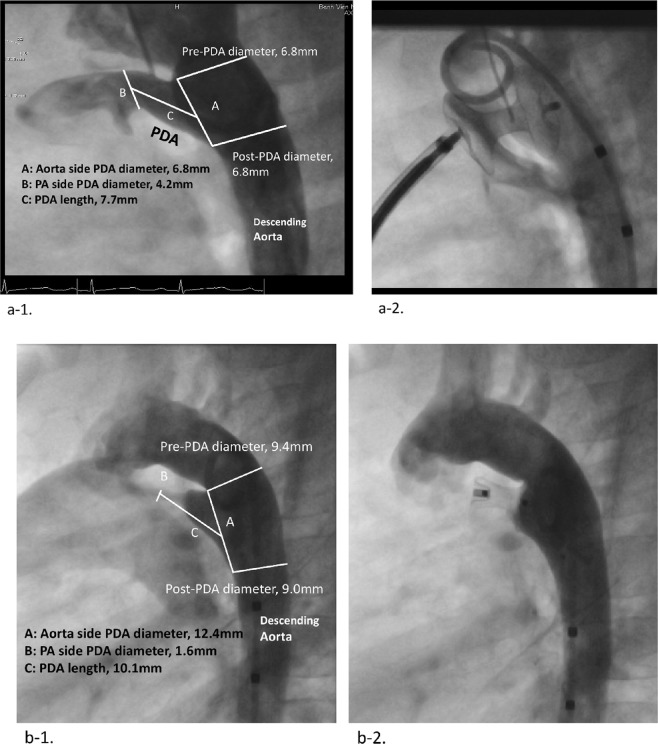
This study investigated the characteristics of congenital rubella syndrome (CRS)-associated cardiac complications, particularly patent ductus arteriosus (PDA). We reviewed the medical records of patients with CRS who were admitted to the Children's Hospital 1 in Vietnam between December 2010 and December 2012, and patients with CRS who underwent PDA transcatheter occlusion therapy at the cardiology department between December 2009 and December 2015. We compared the characteristics of PDA treated with transcatheter closure between children with CRS (CRS-PDA) and those without CRS (non-CRS-PDA) who underwent PDA transcatheter closure between July 2014 and December 2015. One-hundred-and-eight children with CRS were enrolled. Cardiac defects (99%), cataracts (72%), and hearing impairment (7%) were detected. Fifty CRS-PDA and 290 non-CRS-PDA patients were examined. CRS-PDA patients had smaller median birthweight (p < 0.001), more frequent pulmonary (p < 0.001) and aortic stenosis (p < 0.001), higher main pulmonary artery pressure, and higher aortic pressure in systole/diastole (p < 0.001 for each) than did non-CRS-PDA patients. The proportion of tubular-type PDA was higher in CRS-PDA patients (16%) than in non-CRS-PDA patients (3%) (p = 0.020). Tubular-type PDA was frequently seen in patients with CRS and accompanied by pulmonary/systemic hypertension and pulmonary/aortic stenosis; in these patients, more cautious device selection is needed for transcatheter PDA closure.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
