

Progress in Documented Early Identification and Intervention for Deaf and Hard of Hearing Infants: CDC's Hearing Screening and Follow-up Survey, United States, 2006-2016
- PMID: 31745502
- PMCID: PMC6863447
- DOI: 10.26077/6sj1-mw42
Progress in Documented Early Identification and Intervention for Deaf and Hard of Hearing Infants: CDC's Hearing Screening and Follow-up Survey, United States, 2006-2016
Abstract
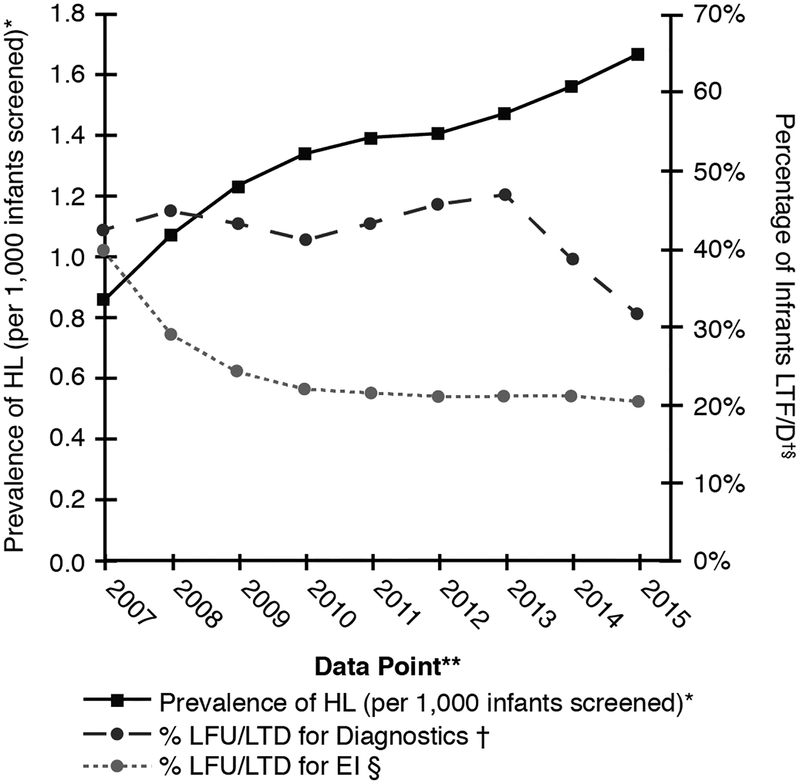
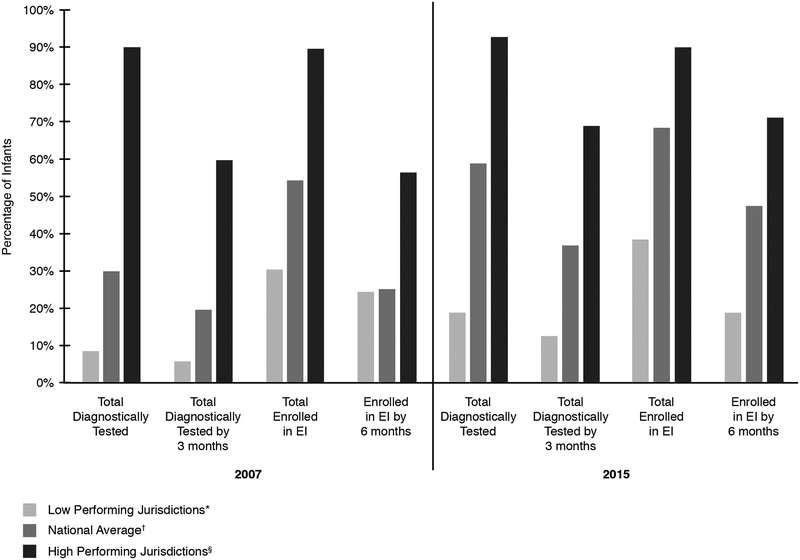
The national EHDI 1-3-6 goals state that all infants should be screened for hearing loss before 1 month of age; with diagnostic testing before 3 months of age for those who do not pass screening; and early intervention (EI) services before 6 months of age for those with permanent hearing loss. This report updates previous summaries of progress on these goals by U.S. states and territories. Data are based on the Hearing Screening and Follow-up Survey (HSFS) conducted annually by the Centers for Disease Control and Prevention for the years 2006-2016. Trends were assessed using 3-year moving averages, with rates of newborns lost to follow-up or lost to documentation (LTF/D) also examined. During this period, the percentage of infants screened before one month increased from 85.1% to 95.3%, while the percentage receiving diagnostic testing before three months increased from 19.8% to 36.6%, and the percentage of infants identified with permanent hearing loss enrolled in early intervention (EI) before six months increased from 25.1% to 47.2%. Percentages of infants who ultimately received screening, diagnostic testing, and early intervention services - regardless of timing - were higher. During this period, LTF/D declined from 42.1% to 31.3% for diagnostic testing, and 39.4% to 20.3% for EI services. Diagnoses of hearing loss recorded increased from 0.9 to 1.7 per 1,000 infants screened, likely reflecting improved data.
Figures
References
-
- Centers for Disease Control and Prevention. (2003). Infants tested for hearing loss-United States, 1999–2001. MMWR. Morbidity and Mortality Weekly Report, 52(41), 981–984. - PubMed
-
- Elssmann S, Matkin N, & Sabo M (1987). Early identification of congenital sensorineural hearing impairment. The Hearing Journal, 40(9), 13–17.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous