

Surgical versus Medical Castration for Metastatic Prostate Cancer: Use and Overall Survival in a National Cohort
- PMID: 31746656
- PMCID: PMC7145732
- DOI: 10.1097/JU.0000000000000684
Surgical versus Medical Castration for Metastatic Prostate Cancer: Use and Overall Survival in a National Cohort
Abstract
Purpose: Surgical castration for metastatic prostate cancer is used less frequently than medical castration yet costs less, requires less followup and may be associated with fewer adverse effects. We evaluated temporal trends and factors associated with the use of surgical castration.
Materials and methods: This retrospective cohort study sampled 24,805 men with newly diagnosed (de novo) metastatic prostate cancer from a national cancer registry in the United States (2004 to 2016). Multivariable logistic regression assessed the association between sociodemographic factors and surgery. Multivariable Cox regression evaluated the association between castration type and overall survival.
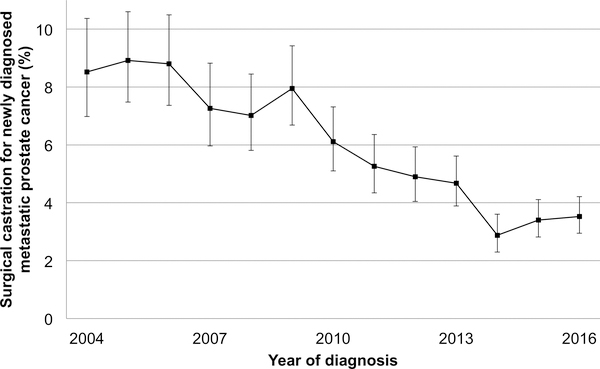
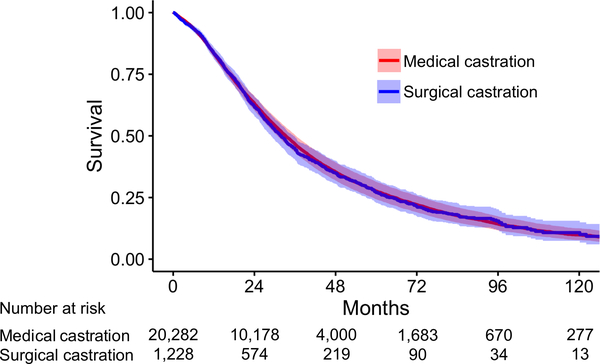
Results: Overall 5.4% of men underwent surgical castration. This figure decreased from 8.5% in 2004 to 3.5% in 2016 (per year later OR 0.89, 95% CI 0.87-0.91, p <0.001). Compared to Medicare, private insurance was associated with less surgery (OR 0.73, 95% CI 0.61-0.87, p <0.001) while Medicaid or no insurance was associated with more surgery (OR 1.68, 95% CI 1.34-2.11, p <0.001 and OR 2.12, 95% CI 1.58-2.85, p <0.001, respectively). Regional median income greater than $63,000 was associated with less surgery (vs income less than $38,000 OR 0.61, 95% CI 0.43-0.85, p=0.004). After a median followup of 30 months castration type was not associated with differences in survival (surgical vs medical HR 1.02, 95% CI 0.95-1.09, p=0.6).
Conclusions: In a contemporary, real-world cohort surgical castration use is low and decreasing despite its potential advantages and similar survival rate compared to medical castration. Men with potentially limited health care access undergo more surgery, perhaps reflecting a provider bias toward the perceived benefit of permanent castration.
Keywords: United States; castration; epidemiology; orchiectomy; prostatic neoplasms.
Conflict of interest statement
Figures
Comment in
-
Editorial Comment.J Urol. 2020 May;203(5):938-939. doi: 10.1097/JU.0000000000000684.01. Epub 2020 Jan 29. J Urol. 2020. PMID: 31994967 No abstract available.
References
-
- Collier A, Ghosh S, McGlynn B et al.: Prostate cancer, androgen deprivation therapy, obesity, the metabolic syndrome, type 2 diabetes, and cardiovascular disease: a review. Am J Clin Oncol, 35: 504, 2012 - PubMed
-
- Smith MR, Lee WC, Brandman J et al.: Gonadotropin-releasing hormone agonists and fracture risk: a claims-based cohort study of men with nonmetastatic prostate cancer. J Clin Oncol, 23: 7897, 2005 - PubMed
-
- Tsai HK, D’Amico AV, Sadetsky N et al.: Androgen deprivation therapy for localized prostate cancer and the risk of cardiovascular mortality. J Natl Cancer Inst, 99: 1516, 2007 - PubMed
-
- Sun M, Choueiri TK, Hamnvik OP et al.: Comparison of Gonadotropin-Releasing Hormone Agonists and Orchiectomy: Effects of Androgen-Deprivation Therapy. JAMA Oncol, 2: 500, 2016 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
