

Incidence Rates and Cumulative Incidences of the Full Spectrum of Diagnosed Mental Disorders in Childhood and Adolescence
- PMID: 31746968
- PMCID: PMC6902162
- DOI: 10.1001/jamapsychiatry.2019.3523
Incidence Rates and Cumulative Incidences of the Full Spectrum of Diagnosed Mental Disorders in Childhood and Adolescence
Abstract
Importance: Knowledge about the epidemiology of mental disorders in children and adolescents is essential for research and planning of health services. Surveys can provide prevalence rates, whereas population-based registers are instrumental to obtain precise estimates of incidence rates and risks.
Objective: To estimate age- and sex-specific incidence rates and risks of being diagnosed with any mental disorder during childhood and adolescence.
Design: This cohort study included all individuals born in Denmark from January 1, 1995, through December 31, 2016 (1.3 million), and followed up from birth until December 31, 2016, or the date of death, emigration, disappearance, or diagnosis of 1 of the mental disorders examined (14.4 million person-years of follow-up). Data were analyzed from September 14, 2018, through June 11, 2019.
Exposures: Age and sex.
Main outcomes and measures: Incidence rates and cumulative incidences of all mental disorders according to the ICD-10 Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research, diagnosed before 18 years of age during the study period.
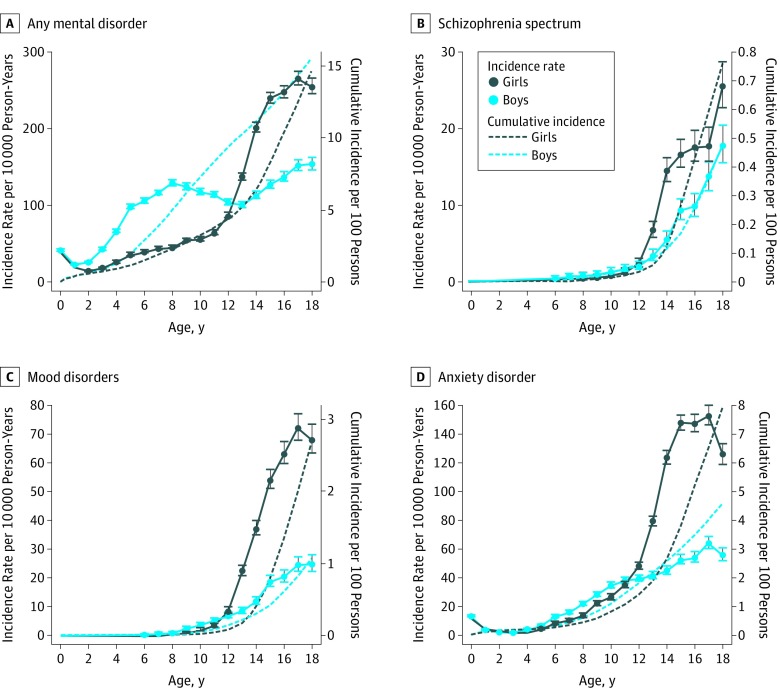
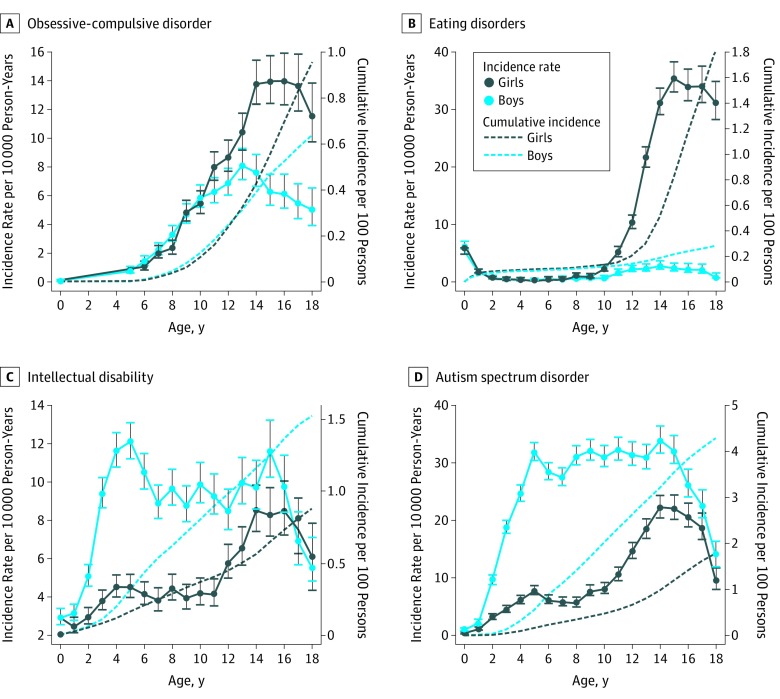
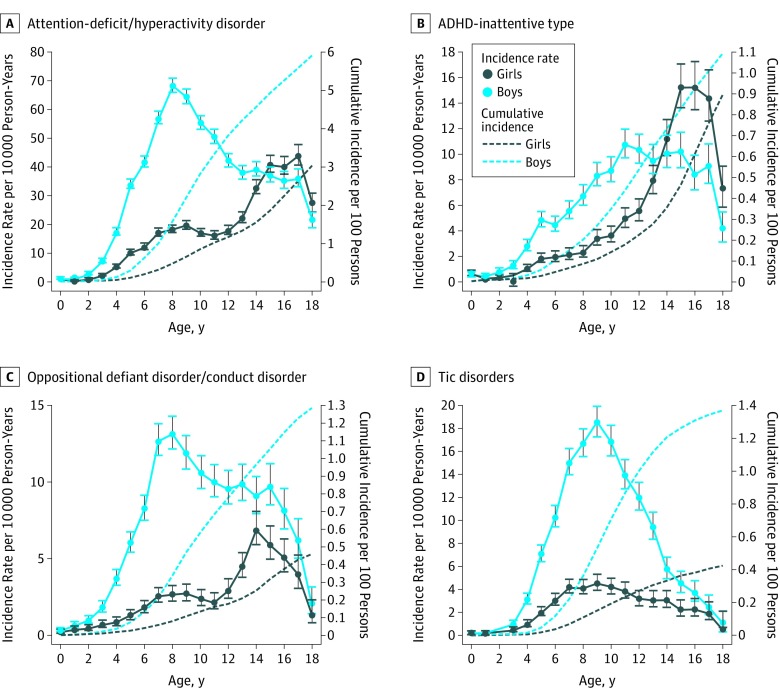
Results: A total of 99 926 individuals (15.01%; 95% CI, 14.98%-15.17%), including 41 350 girls (14.63%; 95% CI, 14.48%-14.77%) and 58 576 boys (15.51%; 95% CI, 15.18%-15.84%), were diagnosed with a mental disorder before 18 years of age. Anxiety disorder was the most common diagnosis in girls (7.85%; 95% CI, 7.74%-7.97%); attention-deficit/hyperactivity disorder (ADHD) was the most common in boys (5.90%; 95% CI, 5.76%-6.03%). Girls had a higher risk than boys of schizophrenia (0.76% [95% CI, 0.72%-0.80%] vs 0.48% [95% CI, 0.39%-0.59%]), obsessive-compulsive disorder (0.96% [95% CI, 0.92%-1.00%] vs 0.63% [95% CI, 0.56%-0.72%]), and mood disorders (2.54% [95% CI, 2.47%-2.61%] vs 1.10% [95% CI, 0.84%-1.21%]). Incidence peaked earlier in boys than girls in ADHD (8 vs 17 years of age), intellectual disability (5 vs 14 years of age), and other developmental disorders (5 vs 16 years of age). The overall risk of being diagnosed with a mental disorder before 6 years of age was 2.13% (95% CI, 2.11%-2.16%) and was higher in boys (2.78% [95% CI, 2.44%-3.15%]) than in girls (1.45% [95% CI, 1.42%-1.49%]).
Conclusions and relevance: This nationwide population-based cohort study provides a first comprehensive assessment of the incidence and risks of mental disorders in childhood and adolescence. By 18 years of age, 15.01% of children and adolescents in this study were diagnosed with a mental disorder. The incidence of several neurodevelopmental disorders peaked in late adolescence in girls, suggesting possible delayed detection. The distinct signatures of the different mental disorders with respect to sex and age may have important implications for service planning and etiological research.
Conflict of interest statement
Figures
References
-
- Naghavi M, Abajobir AA, Abbafati C, et al. ; GBD 2016 Causes of Death Collaborators . Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151-1210. doi: 10.1016/S0140-6736(17)32152-9 - DOI - PMC - PubMed
-
- Institute for Health Metrics and Evaluation (IHME) GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington; 2017. https://vizhub.healthdata.org/gbd-compare. Accessed June 1, 2018.
-
- World Health Organization Mental Health Action Plan 2013-2020. Geneva, Switzerland: World Health Organization; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
