

Setting the Stage for Islet Autoimmunity in Type 2 Diabetes: Obesity-Associated Chronic Systemic Inflammation and Endoplasmic Reticulum (ER) Stress
- PMID: 31748213
- PMCID: PMC7364670
- DOI: 10.2337/dc19-0475
Setting the Stage for Islet Autoimmunity in Type 2 Diabetes: Obesity-Associated Chronic Systemic Inflammation and Endoplasmic Reticulum (ER) Stress
Abstract
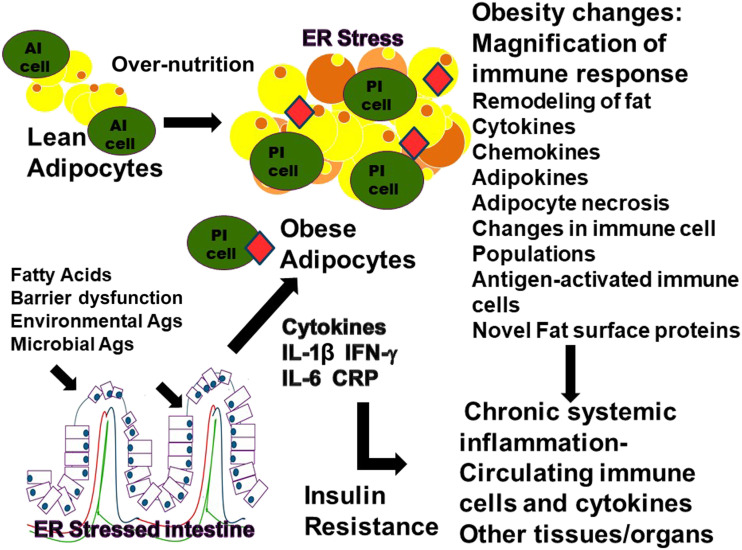
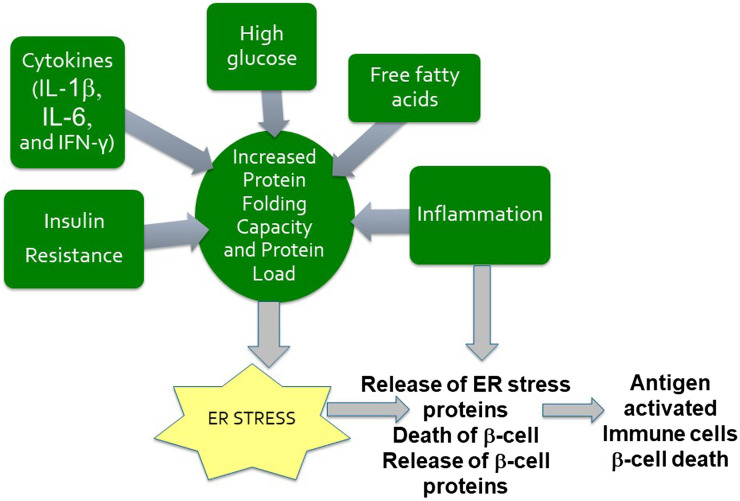
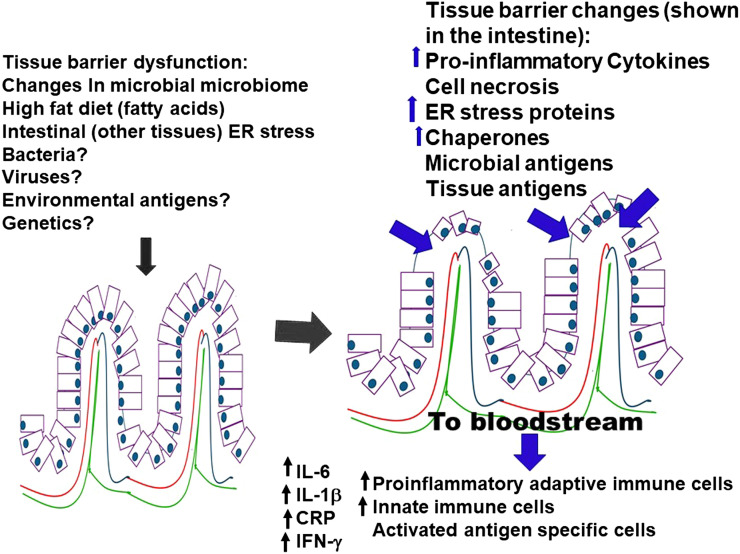
Islet autoimmunity has been identified as a component of both type 1 (T1D) and type 2 (T2D) diabetes, but the pathway through which islet autoimmunity develops in T1D and T2D may be different. Acknowledging the presence of islet autoimmunity in the pathophysiology of T2D, a historically nonautoimmune metabolic disease, would pave the way for important changes in classifications of and therapeutic options for T2D. In order to fully appreciate the importance of islet autoimmunity in T2D, the underlying mechanisms for immune system activation need to be explored. In this review, we focus on the potential origin of immune system activation (innate and adaptive) leading to the development of islet autoimmunity in T2D.
© 2019 by the American Diabetes Association.
Figures

References
-
- Leslie RD, Palmer J, Schloot NC, Lernmark A. Diabetes at the crossroads: relevance of disease classification to pathophysiology and treatment. Diabetologia 2016;59:13–20 - PubMed
-
- Hosszúfalusi N, Vatay A, Rajczy K, et al. . Similar genetic features and different islet cell autoantibody pattern of latent autoimmune diabetes in adults (LADA) compared with adult-onset type 1 diabetes with rapid progression. Diabetes Care 2003;26:452–457 - PubMed
-
- Sladek R, Rocheleau G, Rung J, et al. . A genome-wide association study identifies novel risk loci for type 2 diabetes. Nature 2007;445:881–885 - PubMed
-
- Balasubramanyam A, Garza G, Rodriguez L, et al. . Accuracy and predictive value of classification schemes for ketosis-prone diabetes. Diabetes Care 2006;29:2575–2579 - PubMed
-
- Bingley PJ, Mahon JL, Gale EAM; European Nicotinamide Diabetes Intervention Trial Group . Insulin resistance and progression to type 1 diabetes in the European Nicotinamide Diabetes Intervention Trial (ENDIT). Diabetes Care 2008;31:146–150 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
