Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): multicentre, open label, randomised, superiority trial
- PMID: 31748223
- PMCID: PMC6939660
- DOI: 10.1136/bmj.l6131
Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): multicentre, open label, randomised, superiority trial
Erratum in
-
Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): multicentre, open label, randomised, superiority trial.BMJ. 2021 Dec 15;375:n3072. doi: 10.1136/bmj.n3072. BMJ. 2021. PMID: 34911689 Free PMC article. No abstract available.
Abstract
Objective: To evaluate if induction of labour at 41 weeks improves perinatal and maternal outcomes in women with a low risk pregnancy compared with expectant management and induction of labour at 42 weeks.
Design: Multicentre, open label, randomised controlled superiority trial.
Setting: 14 hospitals in Sweden, 2016-18.
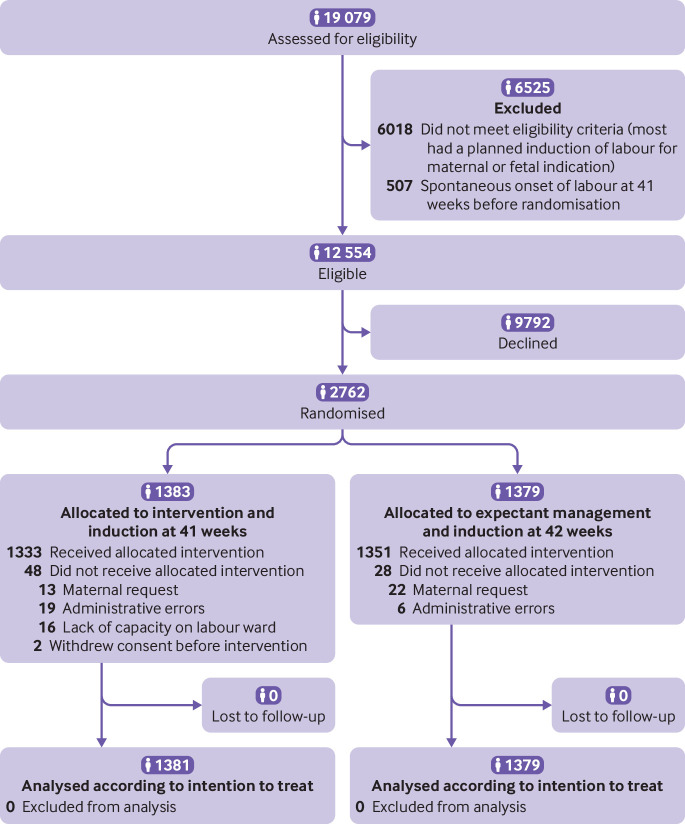
Participants: 2760 women with a low risk uncomplicated singleton pregnancy randomised (1:1) by the Swedish Pregnancy Register. 1381 women were assigned to the induction group and 1379 were assigned to the expectant management group.
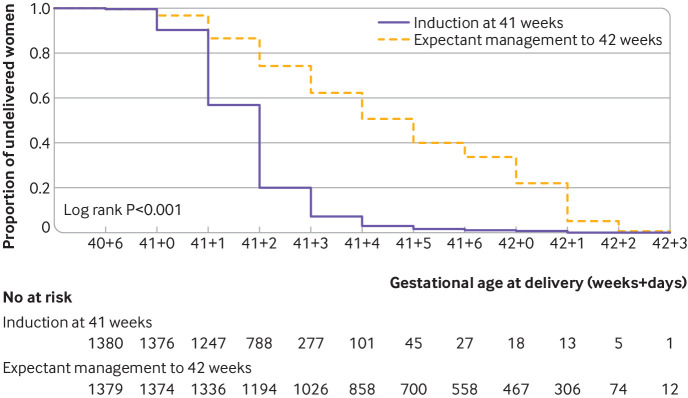
Interventions: Induction of labour at 41 weeks and expectant management and induction of labour at 42 weeks.
Main outcome measures: The primary outcome was a composite perinatal outcome including one or more of stillbirth, neonatal mortality, Apgar score less than 7 at five minutes, pH less than 7.00 or metabolic acidosis (pH <7.05 and base deficit >12 mmol/L) in the umbilical artery, hypoxic ischaemic encephalopathy, intracranial haemorrhage, convulsions, meconium aspiration syndrome, mechanical ventilation within 72 hours, or obstetric brachial plexus injury. Primary analysis was by intention to treat.
Results: The study was stopped early owing to a significantly higher rate of perinatal mortality in the expectant management group. The composite primary perinatal outcome did not differ between the groups: 2.4% (33/1381) in the induction group and 2.2% (31/1379) in the expectant management group (relative risk 1.06, 95% confidence interval 0.65 to 1.73; P=0.90). No perinatal deaths occurred in the induction group but six (five stillbirths and one early neonatal death) occurred in the expectant management group (P=0.03). The proportion of caesarean delivery, instrumental vaginal delivery, or any major maternal morbidity did not differ between the groups.
Conclusions: This study comparing induction of labour at 41 weeks with expectant management and induction at 42 weeks does not show any significant difference in the primary composite adverse perinatal outcome. However, a reduction of the secondary outcome perinatal mortality is observed without increasing adverse maternal outcomes. Although these results should be interpreted cautiously, induction of labour ought to be offered to women no later than at 41 weeks and could be one (of few) interventions that reduces the rate of stillbirths.
Trial registration: Current Controlled Trials ISRCTN26113652.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationship with any organisation that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. AKW has received free reagents (PlGF) from Roche for a prediction study of pre-eclampsia.
Figures