

Therapeutic strategies for diffuse midline glioma from high-throughput combination drug screening
- PMID: 31748226
- PMCID: PMC7132630
- DOI: 10.1126/scitranslmed.aaw0064
Therapeutic strategies for diffuse midline glioma from high-throughput combination drug screening
Abstract
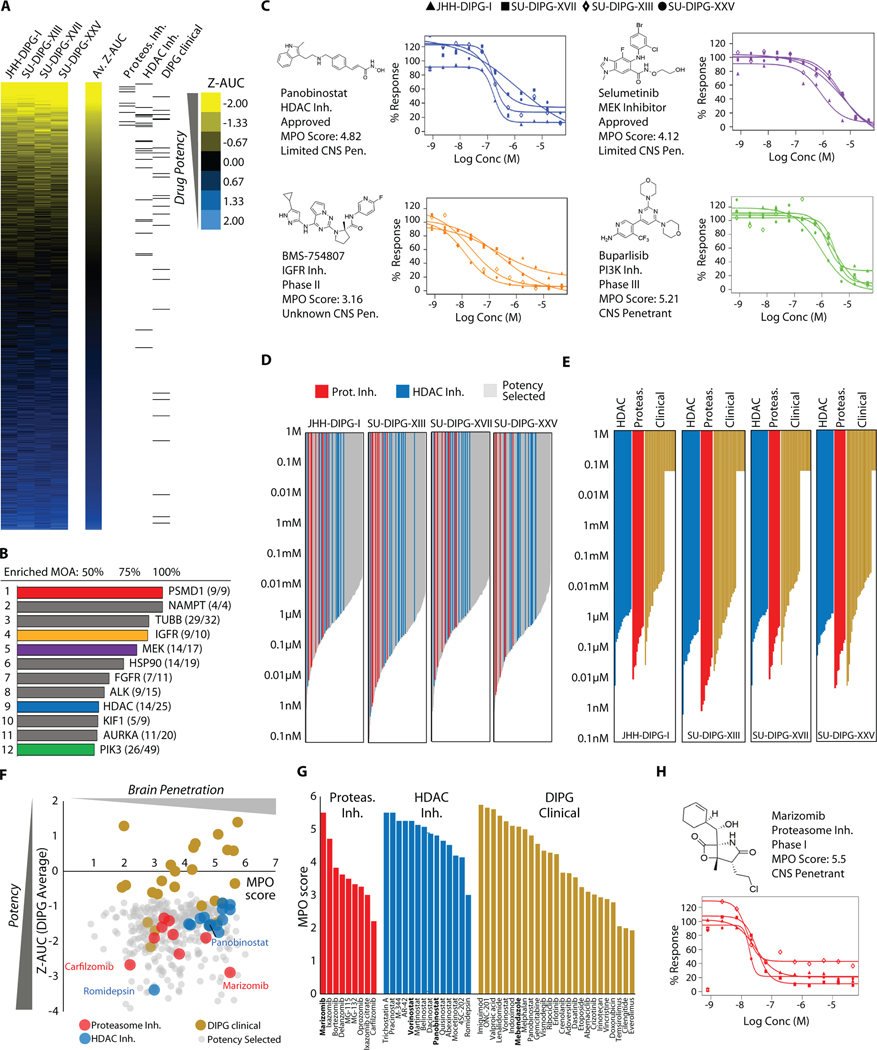
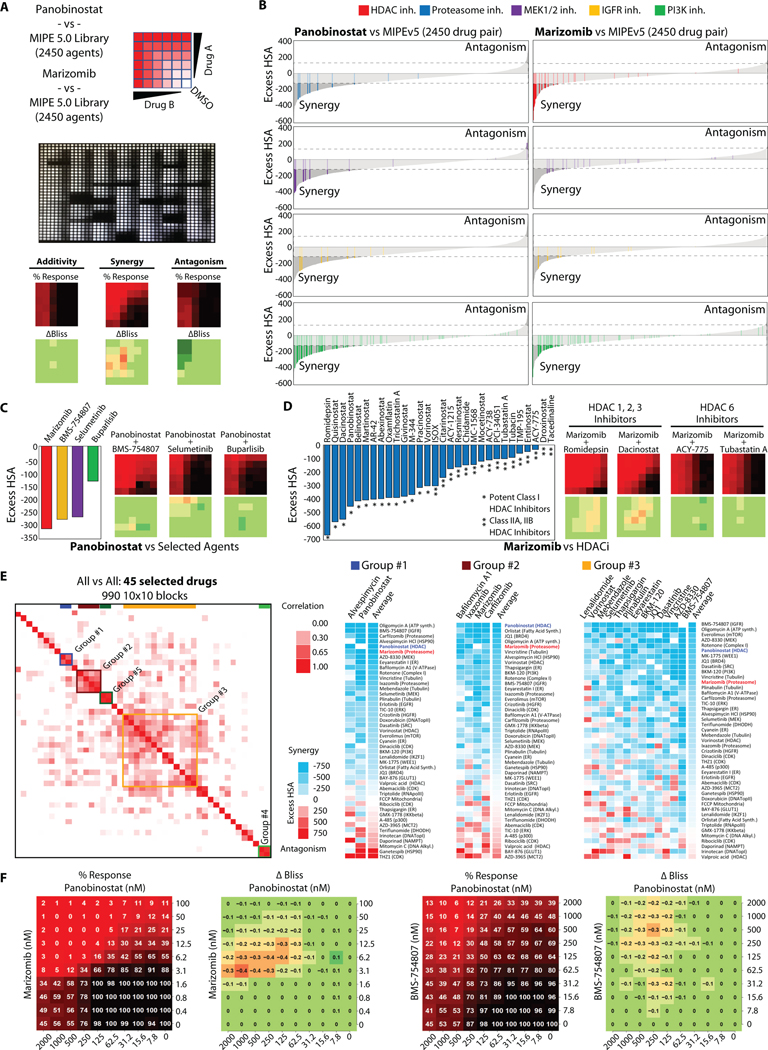
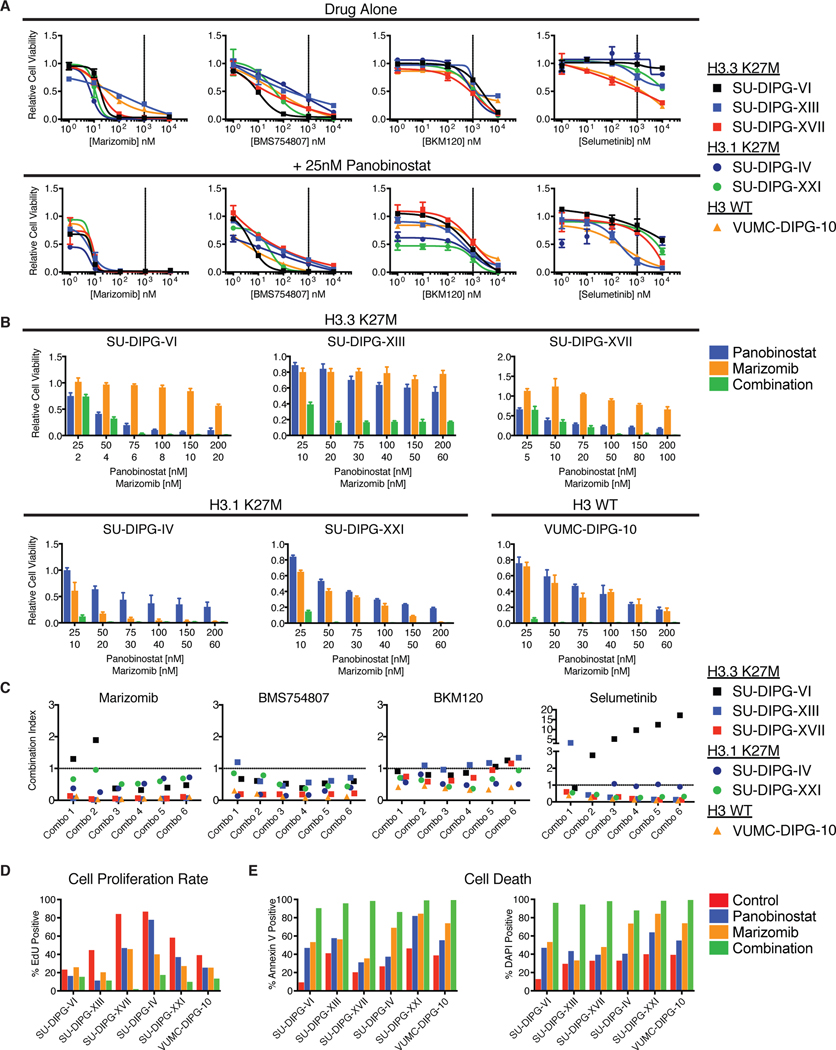
Diffuse midline gliomas (DMGs) are universally lethal malignancies occurring chiefly during childhood and involving midline structures of the central nervous system, including thalamus, pons, and spinal cord. These molecularly related cancers are characterized by high prevalence of the histone H3K27M mutation. In search of effective therapeutic options, we examined multiple DMG cultures in sequential quantitative high-throughput screens (HTS) of 2706 approved and investigational drugs. This effort generated 19,936 single-agent dose responses that inspired a series of HTS-enabled drug combination assessments encompassing 9195 drug-drug examinations. Top combinations were validated across patient-derived cell cultures representing the major DMG genotypes. In vivo testing in patient-derived xenograft models validated the combination of the multi-histone deacetylase (HDAC) inhibitor panobinostat and the proteasome inhibitor marizomib as a promising therapeutic approach. Transcriptional and metabolomic surveys revealed substantial alterations to key metabolic processes and the cellular unfolded protein response after treatment with panobinostat and marizomib. Mitigation of drug-induced cytotoxicity and basal mitochondrial respiration with exogenous application of nicotinamide mononucleotide (NMN) or exacerbation of these phenotypes when blocking nicotinamide adenine dinucleotide (NAD+) production via nicotinamide phosphoribosyltransferase (NAMPT) inhibition demonstrated that metabolic catastrophe drives the combination-induced cytotoxicity. This study provides a comprehensive single-agent and combinatorial drug screen for DMG and identifies concomitant HDAC and proteasome inhibition as a promising therapeutic strategy that underscores underrecognized metabolic vulnerabilities in DMG.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures



References
-
- Jansen MHA, Van Vuurden DG, Vandertop WP, Kaspers GJL, Diffuse intrinsic pontine gliomas: a systematic update on clinical trials and biology, Cancer Treat Rev. 38, 27–35 (2012). - PubMed
-
- Cooney T, Lane A, Bartels U, Bouffet E, Goldman S, Leary SES, Foreman NK, Packer RJ, Broniscer A, Minturn JE, Shih CS, Chintagumpala M, Hassall T, Gottardo NG, Dholaria H, Hoffman L, Chaney B, Baugh J, Doughman R, Leach JL, Jones BV, Fouladi M, Warren KE, Monje M, Contemporary survival endpoints: an International Diffuse Intrinsic Pontine Glioma Registry study, Neuro-Oncol. 19, 1279–1280 (2017). - PMC - PubMed
-
- Schwartzentruber J, Korshunov A, Liu XY, Jones DT, Pfaff E, Jacob K, Sturm D, Fontebasso AM, Quang DA, Tönjes M, Hovestadt V, Albrecht S, Kool M, Nantel A, Konermann C, Lindroth A, Jäger N, Rausch T, Ryzhova M, Korbel JO, Hielscher T, Hauser P, Garami A. Klekner, Bognar L, Ebinger M, Schuhmann MU, Scheurlen W, Pekrun A, Frühwald MC, Roggendorf W, Kramm C, Dürken M, Atkinson J, Lepage P, Montpetit A, Zakrzewska M, Zakrzewski K, Liberski PP, Dong Z, Siegel P, Kulozik AE, Zapatka M, Guha A, Malkin D, Felsberg J, Reifenberger G, von Deimling A, Ichimura K, Collins VP, Witt H, Milde T, Witt O, Zhang C, Castelo-Branco P, Lichter P, Faury D, Tabori U, Plass C, Majewski J, Pfister SM, Jabado N, Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma, Nature 482, 226–31 (2012). - PubMed
-
- Khuong-Quang DA, Buczkowicz P, Rakopoulos P, Liu XY, Fontebasso AM, Bouffet E, Bartels U, Albrecht S, Schwartzentruber J, Letourneau L, Bourgey M, Bourque G, Montpetit A, Bourret G, Lepage P, Fleming A, Lichter P, Kool M, von Deimling A, Sturm D, Korshunov A, Faury D, Jones DT, Majewski J, Pfister SM, Jabado N, Hawkins C, K27M mutation in histone H3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas, Acta Neuropathol 124, 439–447 (2012). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
