

Longitudinal molecular trajectories of diffuse glioma in adults
- PMID: 31748746
- PMCID: PMC6897368
- DOI: 10.1038/s41586-019-1775-1
Longitudinal molecular trajectories of diffuse glioma in adults
Abstract
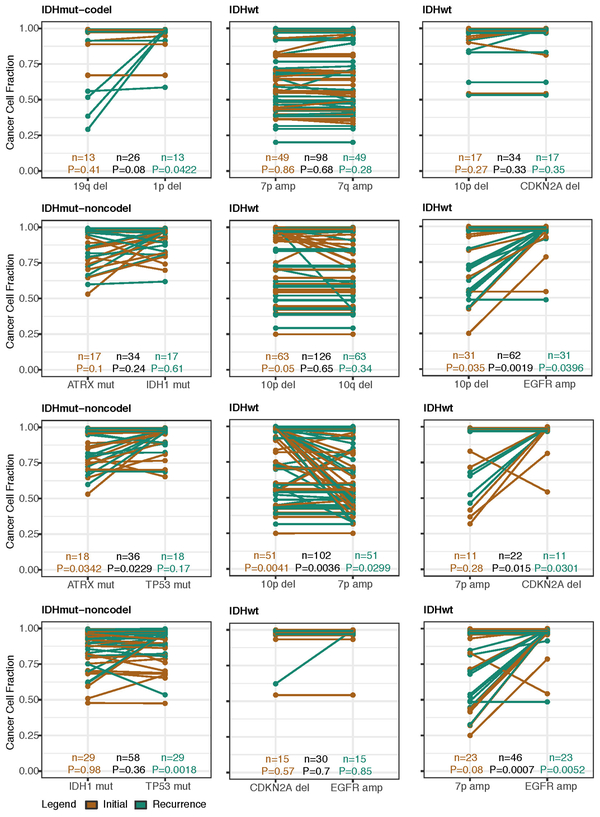
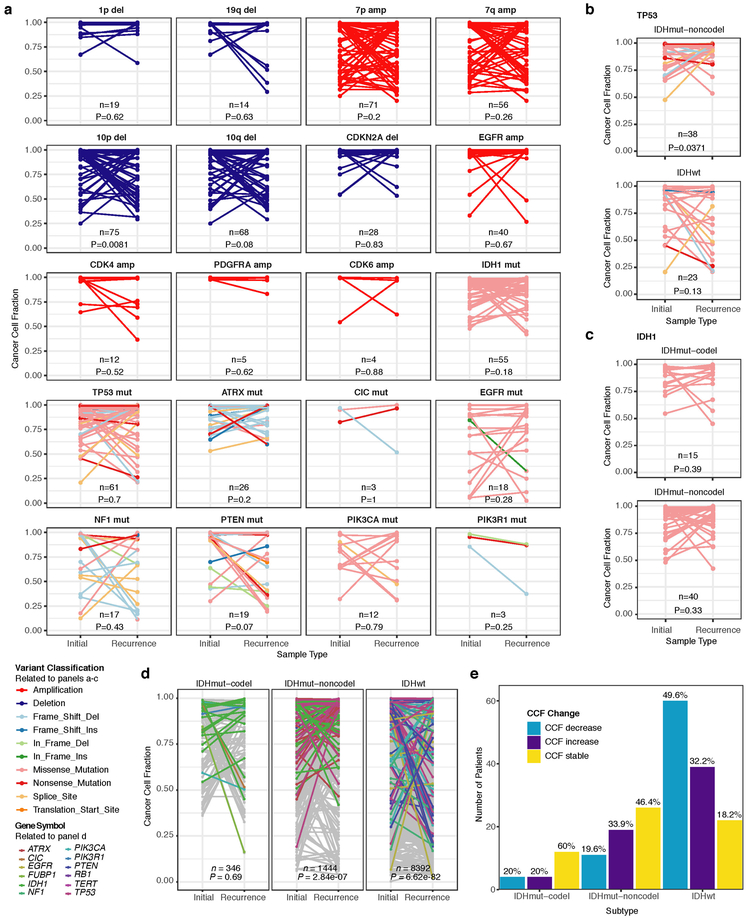
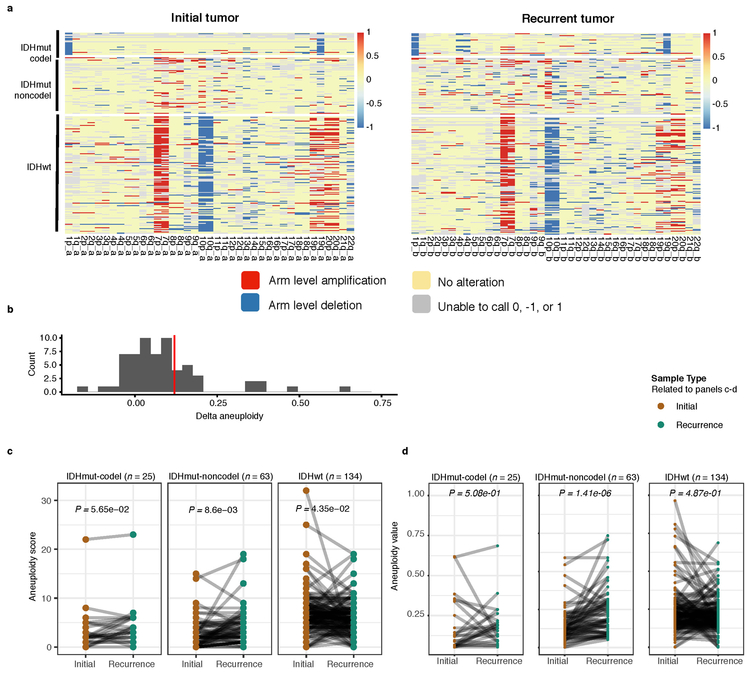
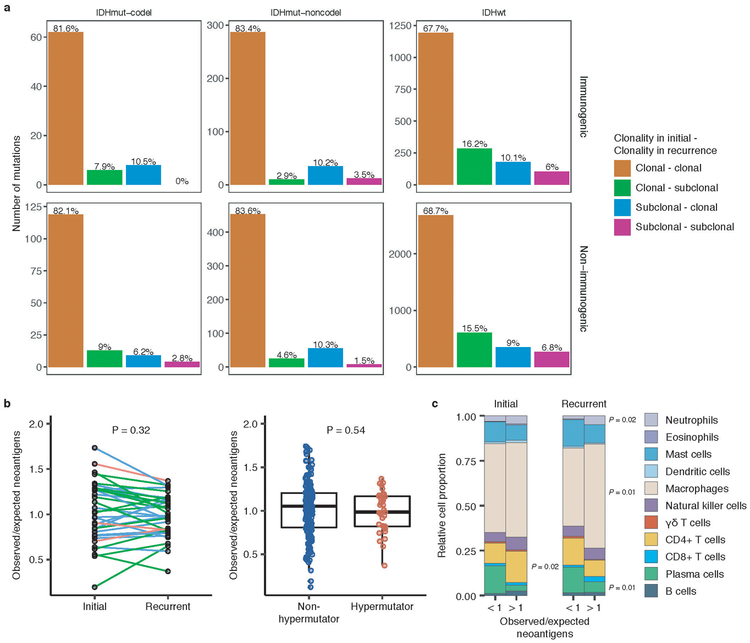
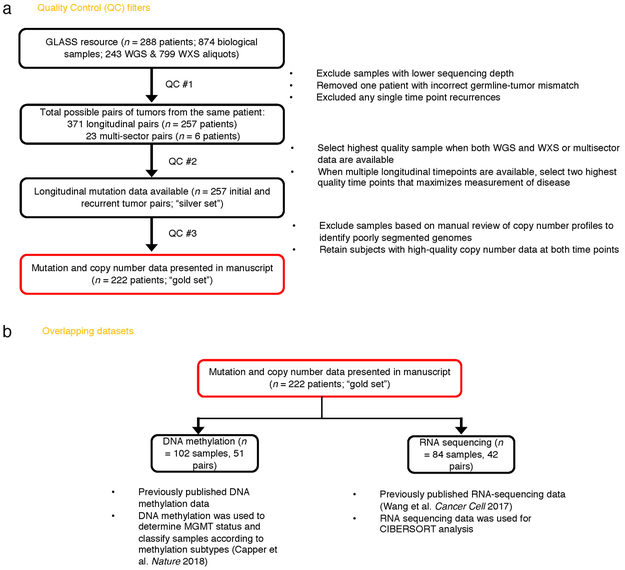
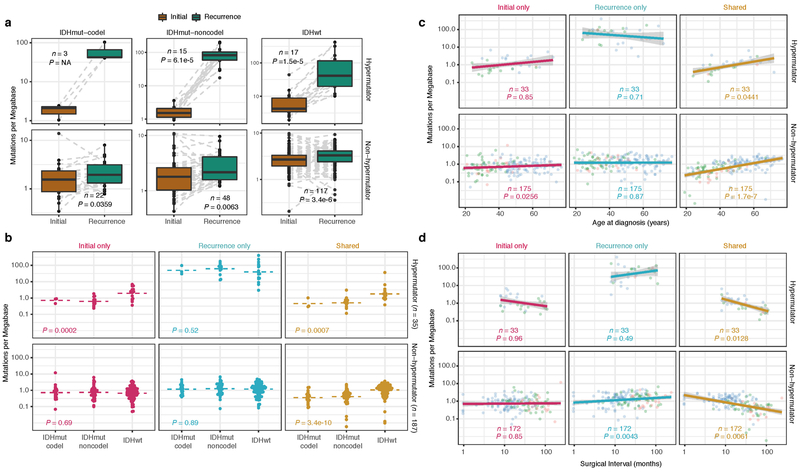
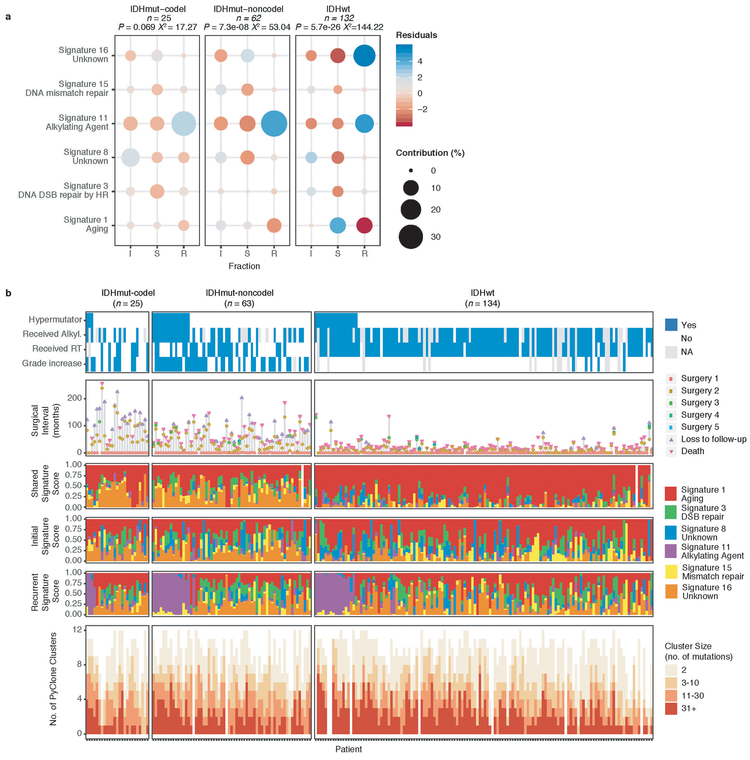
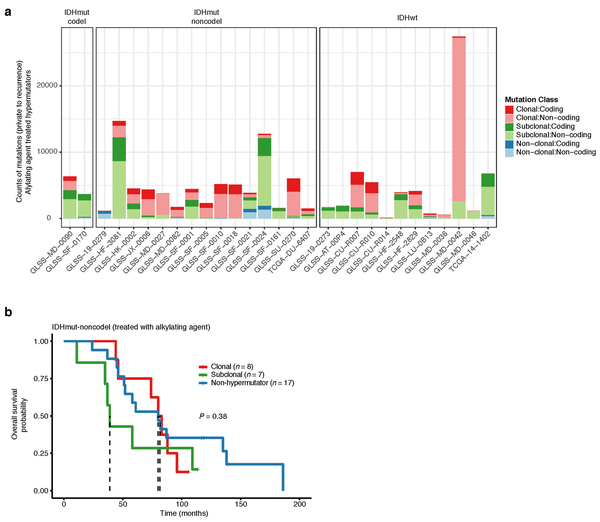
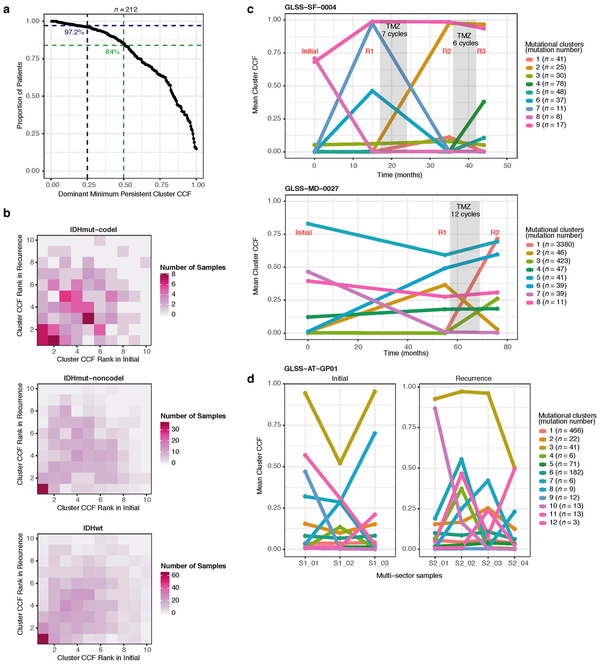
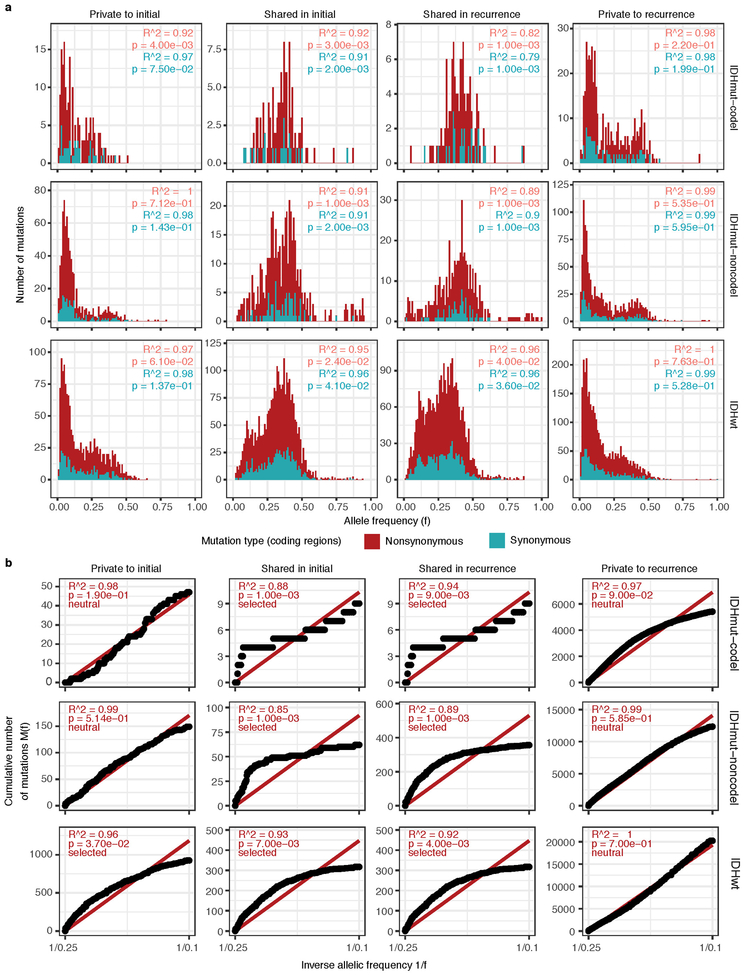
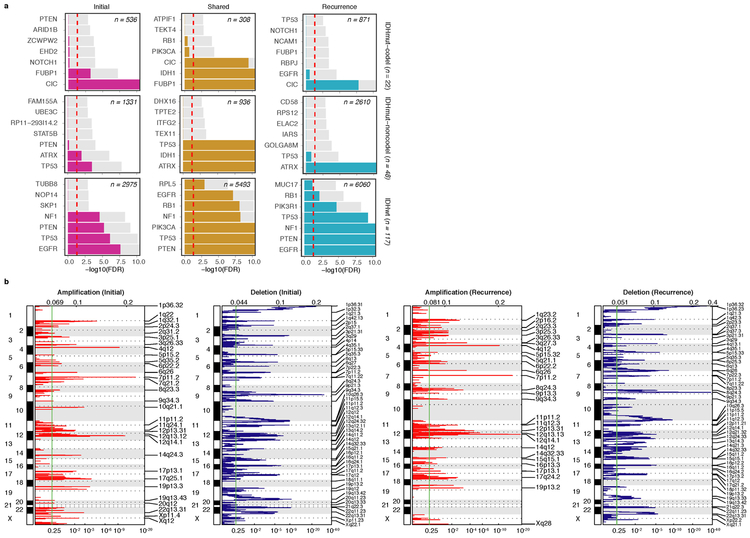
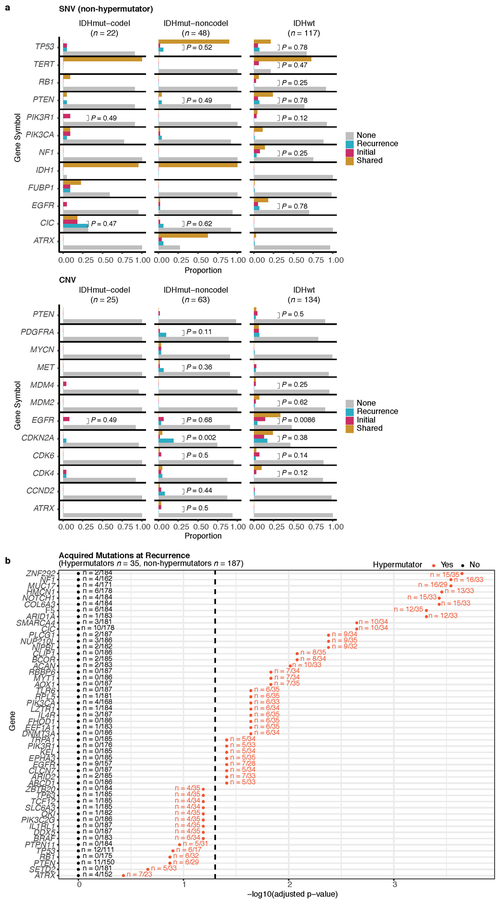
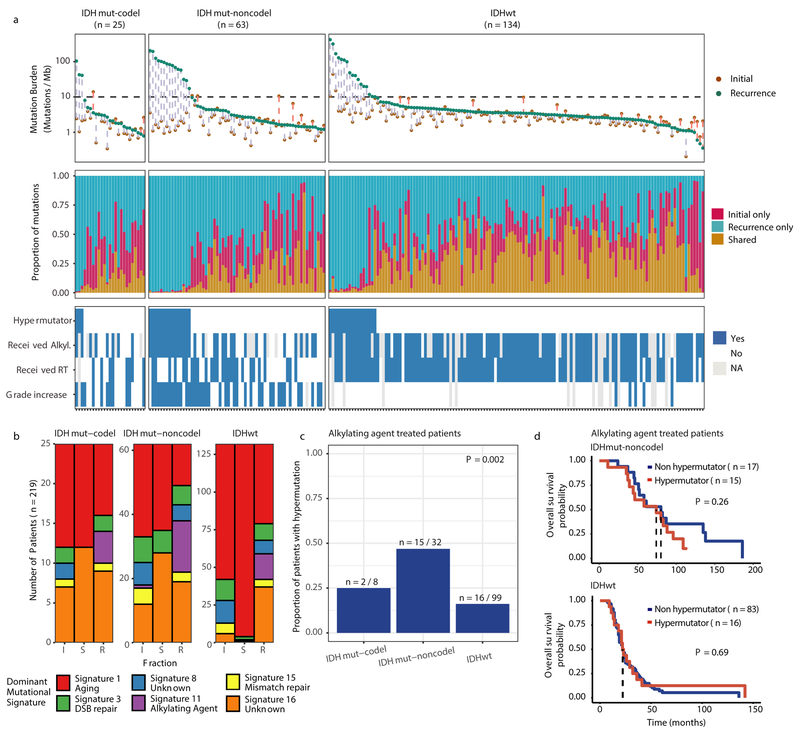
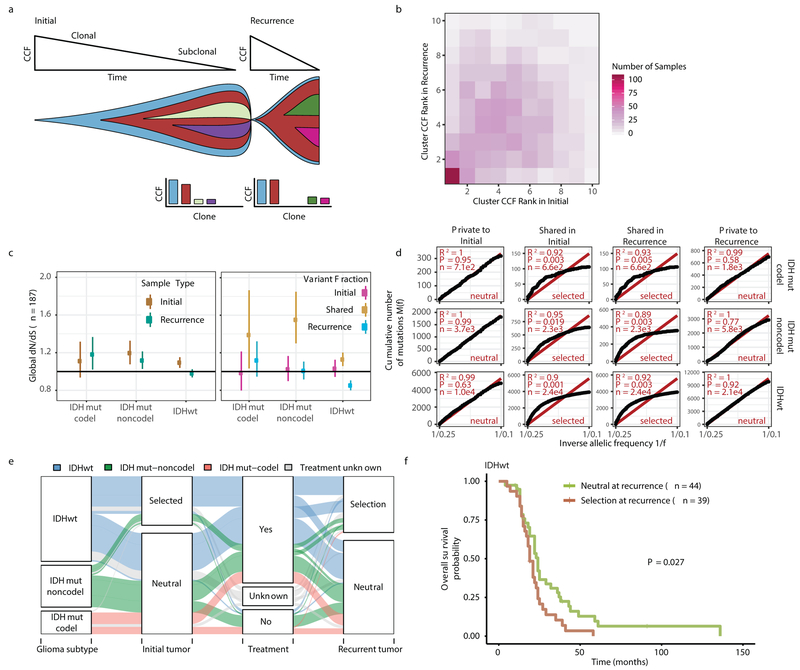
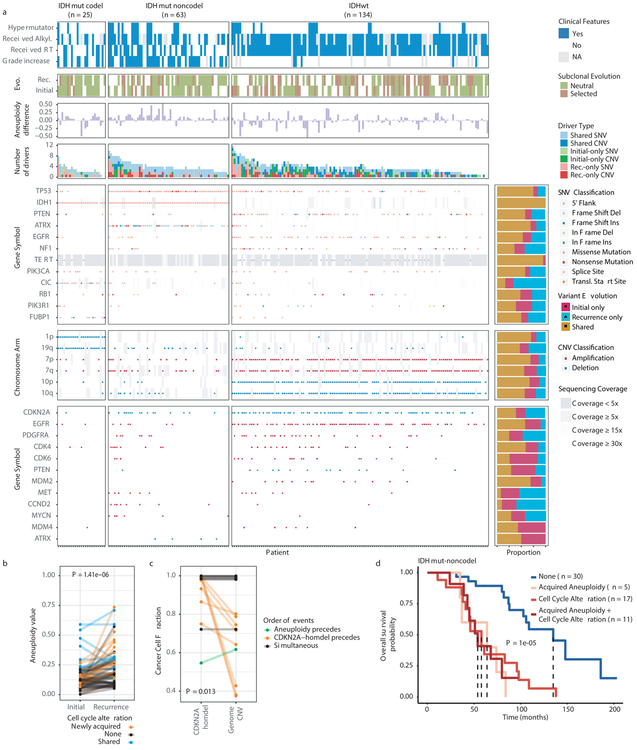
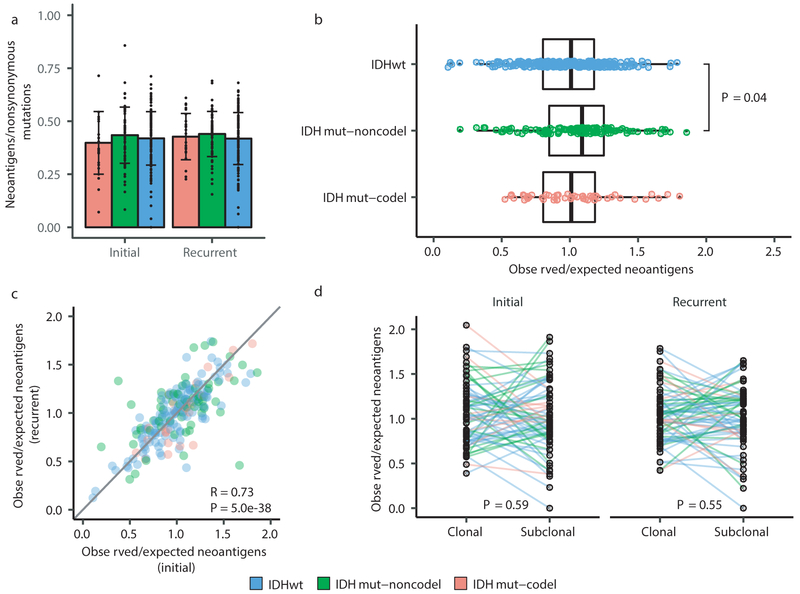
The evolutionary processes that drive universal therapeutic resistance in adult patients with diffuse glioma remain unclear1,2. Here we analysed temporally separated DNA-sequencing data and matched clinical annotation from 222 adult patients with glioma. By analysing mutations and copy numbers across the three major subtypes of diffuse glioma, we found that driver genes detected at the initial stage of disease were retained at recurrence, whereas there was little evidence of recurrence-specific gene alterations. Treatment with alkylating agents resulted in a hypermutator phenotype at different rates across the glioma subtypes, and hypermutation was not associated with differences in overall survival. Acquired aneuploidy was frequently detected in recurrent gliomas and was characterized by IDH mutation but without co-deletion of chromosome arms 1p/19q, and further converged with acquired alterations in the cell cycle and poor outcomes. The clonal architecture of each tumour remained similar over time, but the presence of subclonal selection was associated with decreased survival. Finally, there were no differences in the levels of immunoediting between initial and recurrent gliomas. Collectively, our results suggest that the strongest selective pressures occur during early glioma development and that current therapies shape this evolution in a largely stochastic manner.
Conflict of interest statement
CONFLICTS OF INTEREST
R.G.W.V. declares equity in Boundless Bio, Inc. M.K. receives research grants from BMS and ABBVie. P.K.B. is a consultant for Lilly, Genentech-Roche, Angiochem and Tesaro. P.K.B. receives institutional funding from Merck and Pfizer and honoraria from Merch and Genentech-Roche. W.K.A.Y serves in a consulting or advisory role at DNAtrix Therapeutics. M.W. receives funding from Acceleron, Actelion, Bayer, Isarna, Merck, Sharp & Dohme, Merck (EMD, Darmstadt), Novocure, OGD2, Pigur and Roche as well as honoraria from BMS, Celldex, Immunocellular Therapeutics, Isarna, Magforce, Merck, Sharp & Dohme, Merck (EMD, Darmstadt), Northwest Biotherapeutics, Novocure, Pfizer, Roche, Teva and Tocagen. G.R. receives funding from Roche and Merck (EMD, Darmstadt) as well as honoraria from AbbVie. M.S. is a central reviewer for Parexel Ltd and honoraria are paid to the institution. G.T. reports personal fees from Bristol-Myers-Squibb, personal fees from AbbVie, personal fees from Novocure, personal fees from Medac, travel grants from Bristol-Myers-Squibb, education grants from Novocure, research grants from Roche Diagnostics, research grants from Medac, membership in the National Steering board of the TIGER NIS (Novocure) and the International Steering board of the ON-TRK NIS (Bayer).
Figures
Comment in
-
The Magnifying GLASS: Longitudinal Analysis of Adult Diffuse Gliomas.Cell. 2020 Feb 6;180(3):407-409. doi: 10.1016/j.cell.2020.01.016. Cell. 2020. PMID: 32032515
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA188228/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- CA170278/CA/NCI NIH HHS/United States
- P30 CA034196/CA/NCI NIH HHS/United States
- K99 CA226387/CA/NCI NIH HHS/United States
- U54 CA193313/CA/NCI NIH HHS/United States
- R01 CA215489/CA/NCI NIH HHS/United States
- R00 CA226387/CA/NCI NIH HHS/United States
- R01 CA219943/CA/NCI NIH HHS/United States
- R01 CA108888/CA/NCI NIH HHS/United States
- R01 NS094615/NS/NINDS NIH HHS/United States
- KLI 394/FWF_/Austrian Science Fund FWF/Austria
- R01 CA190121/CA/NCI NIH HHS/United States
- R21 NS114873/NS/NINDS NIH HHS/United States
- R01 CA179044/CA/NCI NIH HHS/United States
- T32 GM008568/GM/NIGMS NIH HHS/United States
- R01 CA230031/CA/NCI NIH HHS/United States
- R01 CA218144/CA/NCI NIH HHS/United States
- R01 CA222146/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
