

Costimulation Blockade in Kidney Transplant Recipients
- PMID: 31749062
- PMCID: PMC6978297
- DOI: 10.1007/s40265-019-01226-6
Costimulation Blockade in Kidney Transplant Recipients
Abstract
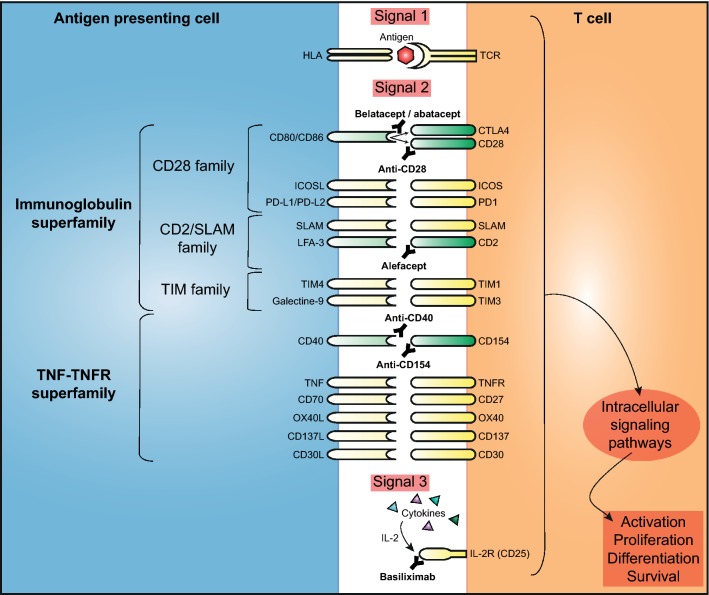
Costimulation between T cells and antigen-presenting cells is essential for the regulation of an effective alloimmune response and is not targeted with the conventional immunosuppressive therapy after kidney transplantation. Costimulation blockade therapy with biologicals allows precise targeting of the immune response but without non-immune adverse events. Multiple costimulation blockade approaches have been developed that inhibit the alloimmune response in kidney transplant recipients with varying degrees of success. Belatacept, an immunosuppressive drug that selectively targets the CD28-CD80/CD86 pathway, is the only costimulation blockade therapy that is currently approved for kidney transplant recipients. In the last decade, belatacept therapy has been shown to be a promising therapy in subgroups of kidney transplant recipients; however, the widespread use of belatacept has been tempered by an increased risk of acute kidney transplant rejection. The purpose of this review is to provide an overview of the costimulation blockade therapies that are currently in use or being developed for kidney transplant indications.
Conflict of interest statement
Dennis A. Hesselink has received grant support, and lecture and consulting fees from Astellas Pharma and Chiesi Pharmaceuticals, as well as lecture fees from Hikma Pharma and grant support from Bristol Myers-Squibb. Martijn W.F van den Hoogen has received grant support from Novartis and Shire, and lecture fees from Astellas Pharma, Chiesi Pharmaceuticals, MSD, Sanofi/Genzyme, Shire and Vifor Pharma. Marieke van der Zwan and Carla C. Baan declare no conflicts of interest.
Figures
Similar articles
-
Belatacept-Resistant Rejection Is Associated With CD28+ Memory CD8 T Cells.Am J Transplant. 2017 Sep;17(9):2285-2299. doi: 10.1111/ajt.14349. Epub 2017 Jul 11. Am J Transplant. 2017. PMID: 28502128 Free PMC article.
-
Increased Pretransplant Frequency of CD28+ CD4+ TEM Predicts Belatacept-Resistant Rejection in Human Renal Transplant Recipients.Am J Transplant. 2017 Sep;17(9):2350-2362. doi: 10.1111/ajt.14350. Epub 2017 Jun 30. Am J Transplant. 2017. PMID: 28502091 Free PMC article.
-
CD28-B7-mediated T cell costimulation in chronic cardiac allograft rejection: differential role of B7-1 in initiation versus progression of graft arteriosclerosis.Am J Pathol. 2001 Mar;158(3):977-86. doi: 10.1016/S0002-9440(10)64044-8. Am J Pathol. 2001. PMID: 11238045 Free PMC article.
-
Belatacept in kidney transplantation.Curr Opin Organ Transplant. 2012 Dec;17(6):640-7. doi: 10.1097/MOT.0b013e32835a4c0d. Curr Opin Organ Transplant. 2012. PMID: 23044530 Review.
-
Belatacept for maintenance immunosuppression in cardiothoracic transplantation: The potential frontier.Clin Transplant. 2018 Oct;32(10):e13363. doi: 10.1111/ctr.13363. Epub 2018 Sep 10. Clin Transplant. 2018. PMID: 30058177 Review.
Cited by
-
New Immunosuppressants in Pediatric Kidney Transplantation: What's in the Pipeline for Kids?Pediatr Transplant. 2025 Feb;29(1):e70008. doi: 10.1111/petr.70008. Pediatr Transplant. 2025. PMID: 39711054 Free PMC article. Review.
-
Monomethyl fumarate prevents alloimmune rejection in mouse heart transplantation by inducing tolerogenic dendritic cells.Acta Biochim Biophys Sin (Shanghai). 2023 May 16;55(5):866-877. doi: 10.3724/abbs.2023088. Acta Biochim Biophys Sin (Shanghai). 2023. PMID: 37184280 Free PMC article.
-
Thrombotic Microangiopathy After Kidney Transplantation: An Underdiagnosed and Potentially Reversible Entity.Front Med (Lausanne). 2021 Apr 8;8:642864. doi: 10.3389/fmed.2021.642864. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33898482 Free PMC article. Review.
-
Comprehensive Phenotyping and Cytokine Production of Circulating B Cells Associate Resting Memory B Cells With Early Antibody-mediated Rejection in Kidney Transplant Recipients.Transplant Direct. 2025 Mar 20;11(4):e1775. doi: 10.1097/TXD.0000000000001775. eCollection 2025 Apr. Transplant Direct. 2025. PMID: 40124243 Free PMC article.
-
Innovative immunosuppression in kidney transplantation: A challenge for unmet needs.World J Transplant. 2022 Mar 18;12(3):27-41. doi: 10.5500/wjt.v12.i3.27. World J Transplant. 2022. PMID: 35433332 Free PMC article. Review.
References
-
- Kasiske BL, Zeier MG, Chapman JR, Craig JC, Ekberg H, Garvey CA, et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: a summary. Kidney Int. 2010;77(4):299–311. - PubMed
-
- Brunet M, van Gelder T, Asberg A, Haufroid V, Hesselink DA, Langman L, et al. Therapeutic drug monitoring of tacrolimus-personalized therapy: second consensus report. Ther Drug Monit. 2019;41(3):261–307. - PubMed
-
- van Gelder T, Hesselink DA. Mycophenolate revisited. Transpl Int. 2015;28(5):508–515. - PubMed
-
- Claes K, Meier-Kriesche HU, Schold JD, Vanrenterghem Y, Halloran PF, Ekberg H. Effect of different immunosuppressive regimens on the evolution of distinct metabolic parameters: evidence from the symphony study. Nephrol Dial Transpl. 2012;27(2):850–857. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
