

Vaccination strategies to control Ebola epidemics in the context of variable household inaccessibility levels
- PMID: 31751337
- PMCID: PMC6894888
- DOI: 10.1371/journal.pntd.0007814
Vaccination strategies to control Ebola epidemics in the context of variable household inaccessibility levels
Abstract
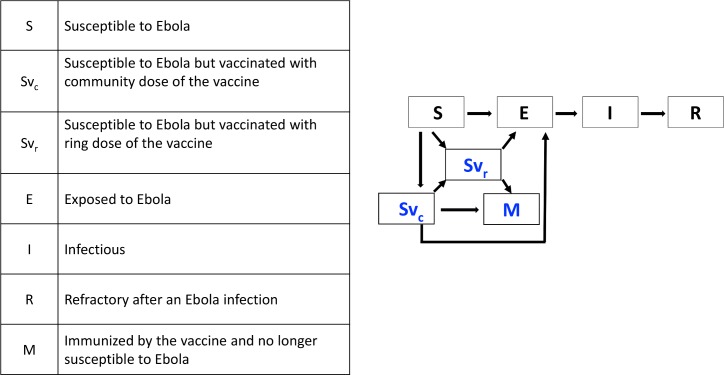
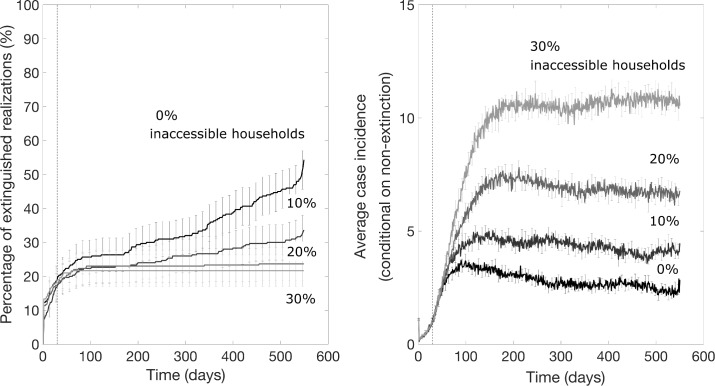
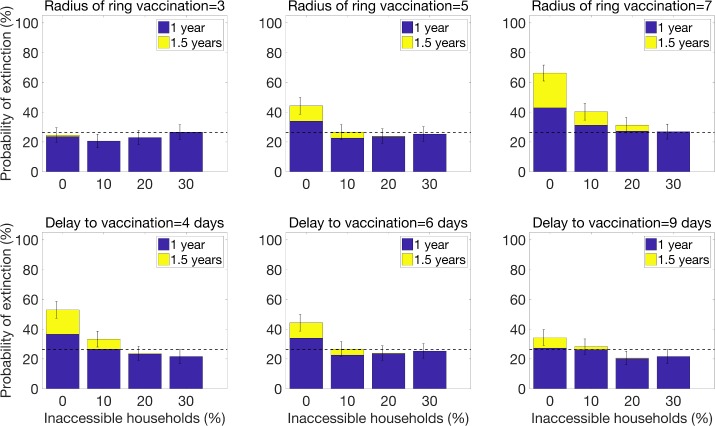
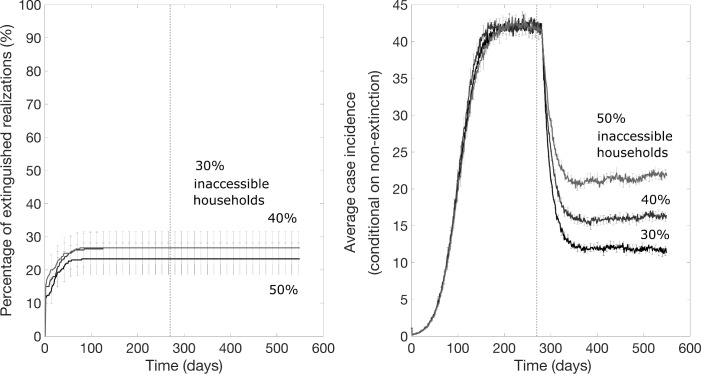
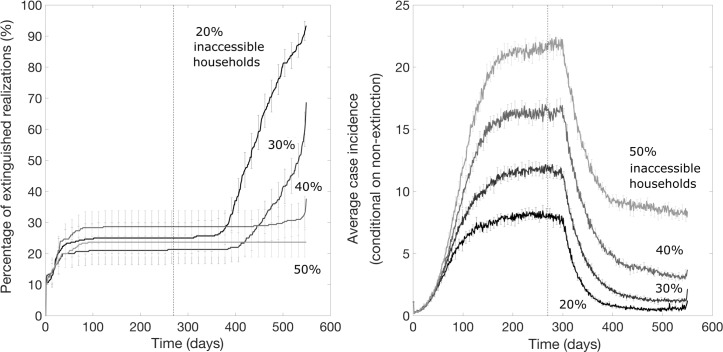
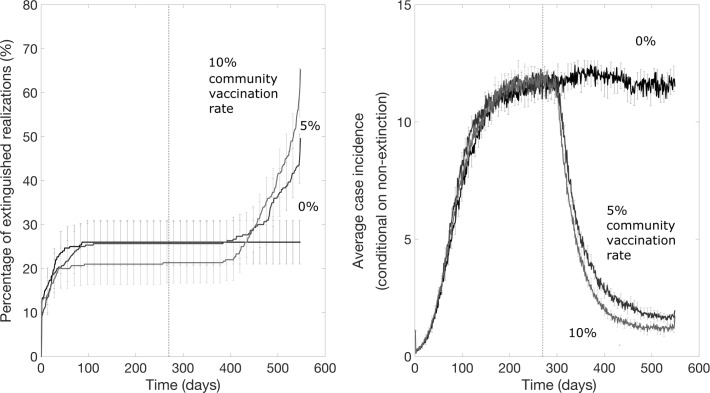
Despite a very effective vaccine, active conflict and community distrust during the ongoing DRC Ebola epidemic are undermining control efforts, including a ring vaccination strategy that requires the prompt immunization of close contacts of infected individuals. However, in April 2019, it was reported 20% or more of close contacts cannot be reached or refuse vaccination, and it is predicted that the ring vaccination strategy would not be effective with such a high level of inaccessibility. The vaccination strategy is now incorporating a "third ring" community-level vaccination that targets members of communities even if they are not known contacts of Ebola cases. To assess the impact of vaccination strategies for controlling Ebola epidemics in the context of variable levels of community accessibility, we employed an individual-level stochastic transmission model that incorporates four sources of heterogeneity: a proportion of the population is inaccessible for contact tracing and vaccination due to lack of confidence in interventions or geographic inaccessibility, two levels of population mixing resembling household and community transmission, two types of vaccine doses with different time periods until immunity, and transmission rates that depend on spatial distance. Our results indicate that a ring vaccination strategy alone would not be effective for containing the epidemic in the context of significant delays to vaccinating contacts even for low levels of household inaccessibility and affirm the positive impact of a supplemental community vaccination strategy. Our key results are that as levels of inaccessibility increase, there is a qualitative change in the effectiveness of the vaccination strategy. For higher levels of vaccine access, the probability that the epidemic will end steadily increases over time, even if probabilities are lower than they would be otherwise with full community participation. For levels of vaccine access that are too low, however, the vaccination strategies are not expected to be successful in ending the epidemic even though they help lower incidence levels, which saves lives, and makes the epidemic easier to contain and reduces spread to other communities. This qualitative change occurs for both types of vaccination strategies: ring vaccination is effective for containing an outbreak until the levels of inaccessibility exceeds approximately 10% in the context of significant delays to vaccinating contacts, a combined ring and community vaccination strategy is effective until the levels of inaccessibility exceeds approximately 50%. More broadly, our results underscore the need to enhance community engagement to public health interventions in order to enhance the effectiveness of control interventions to ensure outbreak containment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Yong E. (2019). The WHO Finally Sounds Its Loudest Alarm Over Ebola in the Congo. The Atlantic. Science.
-
- Frontieres M. S. (2019). Ebola outbreak in Democratic Republic of Congo Fighting an epidemic in a conflict zone. MSF Doctors Without Borders.
-
- 2014 Ebola Outbreak in West Africa—Reported Cases Graphs 2016 [cited 2017 March 23]. Available from: https://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/cumulative-case....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
