

Direct transport vs secondary transfer to level I trauma centers in a French exclusive trauma system: Impact on mortality and determinants of triage on road-traffic victims
- PMID: 31751349
- PMCID: PMC6872206
- DOI: 10.1371/journal.pone.0223809
Direct transport vs secondary transfer to level I trauma centers in a French exclusive trauma system: Impact on mortality and determinants of triage on road-traffic victims
Abstract
Background: Transporting a severely injured patient directly to a trauma center (TC) is consensually considered optimal. Nevertheless, disagreement persists regarding the association between secondary transfer status and outcome. The aim of the study was to compare adjusted mortality between road traffic trauma patients directly or secondarily transported to a level 1 trauma center (TC) in an exclusive French trauma system with a physician staffed prehospital emergency medical system (EMS).
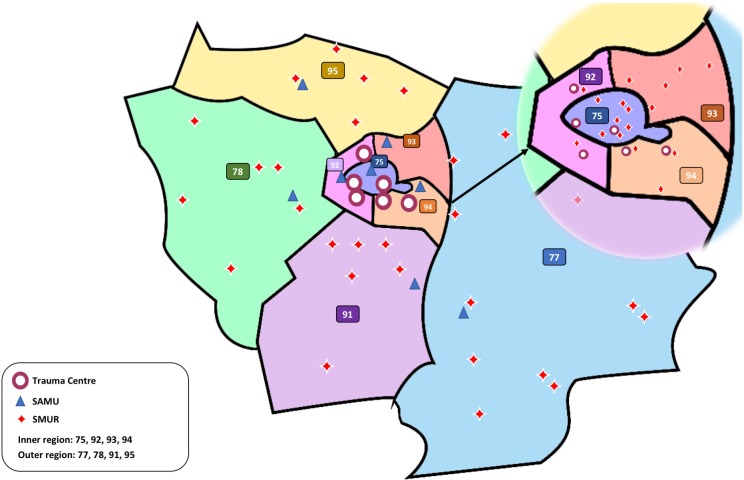
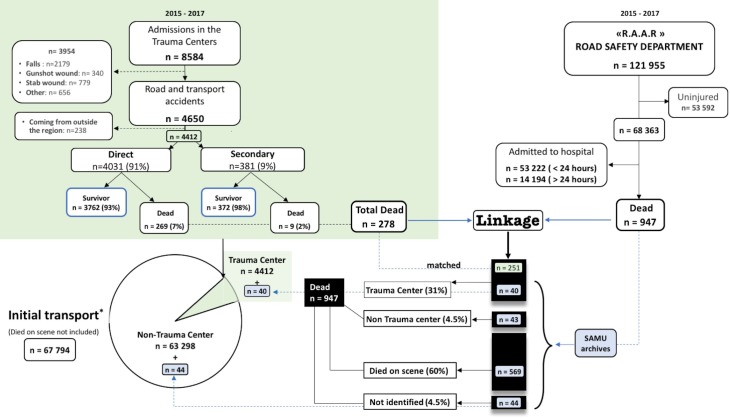
Methods: A retrospective cohort study was performed using 2015-2017 data from a regional trauma registry (Traumabase®), an administrative database on road-traffic accidents and prehospital-EMS records. Multivariate logistic regression models were computed to determine the role of the modality of admission on mortality and to identify factors associated with secondary transfer. The primary outcome was day-30 mortality. Results: During the study period, 121.955 victims of road-traffic accident were recorded among which 4412 trauma patients were admitted in the level 1 regional TCs, 4031 directly and 381 secondarily transferred from lower levels facilities. No significant association between all-cause 30-day mortality and the type of transport was observed (Odds ratio 0.80, 95% confidence interval (CI) [0.3-1.9]) when adjusted for potential confounders. Patients secondarily transferred were older, with low-energy mechanism and presented higher head and abdominal injury scores. Among all 947 death, 43 (4.5%) occurred in lower-level facilities. The population-based undertriage leading to death was 0.15%, 95%CI [0.12-0.19].
Conclusion: In an exclusive trauma system with physician staffed prehospital care, road-traffic victims secondarily transferred to a TC do not have an increased mortality when compared to directly transported patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hay SI, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. 2017;390: 1260–1344. 10.1016/S0140-6736(17)32130-X - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
