

Risk Prediction in Transition: MAGGIC Score Performance at Discharge and Incremental Utility of Natriuretic Peptides
- PMID: 31751788
- PMCID: PMC10062381
- DOI: 10.1016/j.cardfail.2019.11.016
Risk Prediction in Transition: MAGGIC Score Performance at Discharge and Incremental Utility of Natriuretic Peptides
Abstract
Background: Risk stratification for hospitalized patients with heart failure (HF) remains a critical need. The Meta-Analysis Global Group in Chronic Heart Failure (MAGGIC) score is a robust model derived from patients with ambulatory HF. Its validity at the time of discharge and the incremental value of natriuretic peptides (NPs) in this setting is unclear.
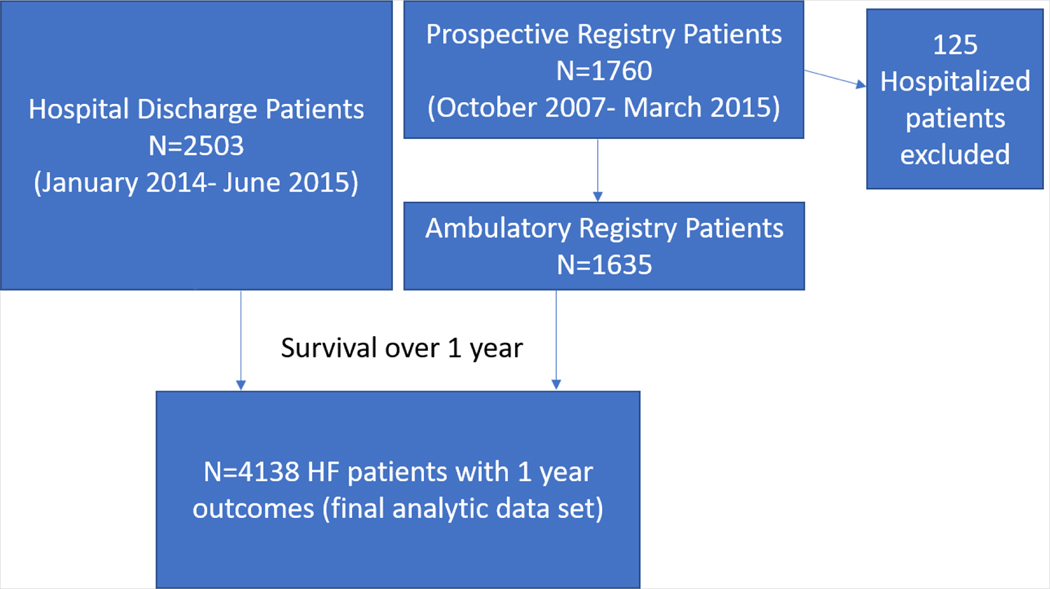
Methods: This was a single-center study examining a total of 4138 patients with HF from 2 groups; hospital discharge patients from administrative data (n = 2503, 60.5%) and a prospective registry of patients with ambulatory HF (n = 1635, 39.5%). The ambulatory registry patients underwent N-terminal pro-B-type NP (BNP) measurement at enrollment, and in the hospitalize discharge cohort clinical BNP levels were abstracted. The primary endpoint was all-cause mortality within 1 year. MAGGIC score performance was compared between cohorts utilizing Cox regression and calibration plots. The incremental value of NPs was assessed using calculated area under the curve and net reclassification improvement (NRI).
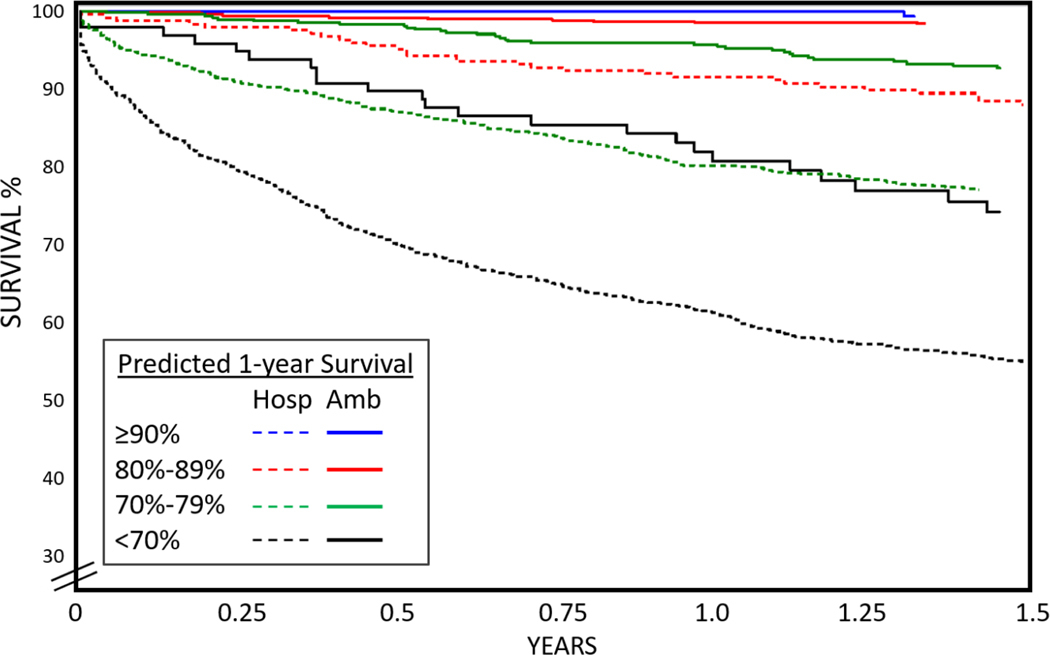
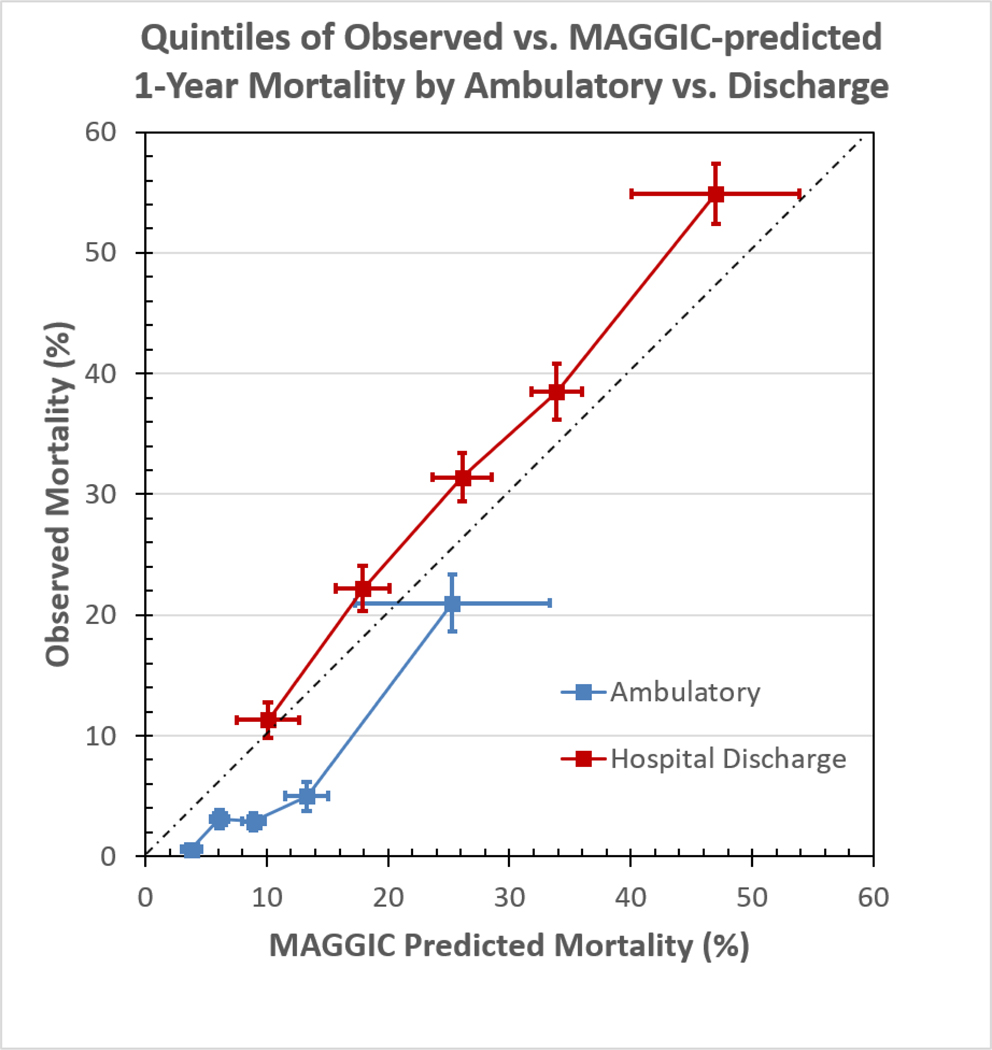
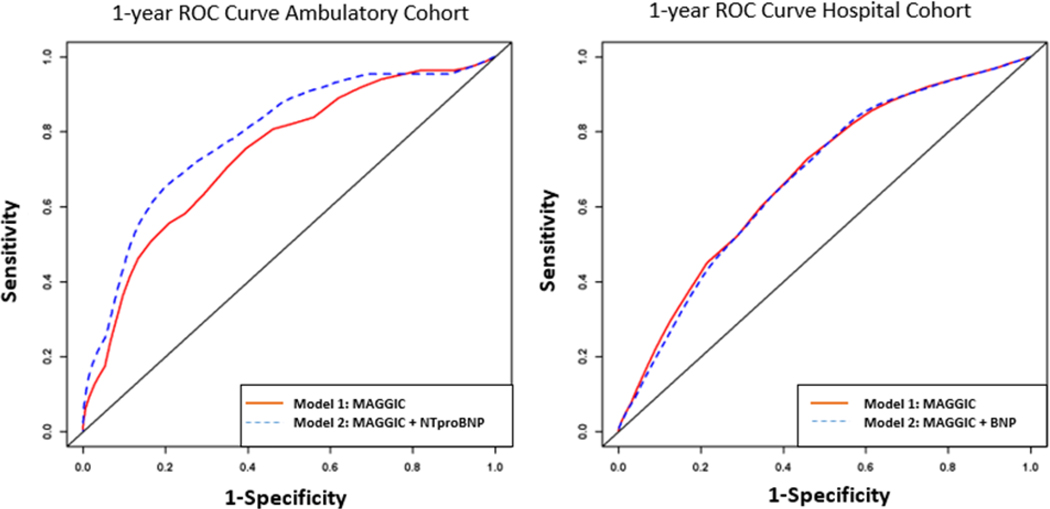
Results: The hospitalized and ambulatory cohorts differed with respect to primary outcome (777 and 100 deaths, respectively), sex (52.1% vs 41.7% female) and race (35% vs 49.5% African American). The MAGGIC score showed poor discrimination of mortality risk in the hospital discharge (C statistic: 0.668, hazard ratio [HR]: 1.1 per point, 95% confidence interval [CI]: 0.652, 0.684) but fair discrimination in the ambulatory cohorts (C statistic: 0.784, HR: 1.16 per point, 95% CI: 0.74, 0.83), respectively, a difference that was statistically significant (P = .001 for C statistic, 0.002 for HR). Calibration assessment indicated that the slope and intercept (of MAGGIC-predicted to observed mortality) did not statistically differ from ideal in either cohort and did not differ between the cohorts (all P > .1). NP levels did not significantly improve prediction in the hospitalized cohort (P = .127) but did in the ambulatory cohort (C statistic: 0.784 [95% CI: 0.74, 0.83] vs 0.82 [95% CI: 0.78, 0.85]; P = .018) with a favorable NRI of 0.354 (95% CI: 0.202-0.469; P = .002).
Conclusion: The MAGGIC score showed poor discrimination when used in patients with HF at hospital discharge, which was inferior to its performance in patients with ambulatory HF. Discrimination within the hospital discharge group was not improved by including hospital NP levels.
Keywords: Heart failure; mortality; risk prediction.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Validation of the MAGGIC (Meta-Analysis Global Group in Chronic Heart Failure) heart failure risk score and the effect of adding natriuretic peptide for predicting mortality after discharge in hospitalized patients with heart failure.PLoS One. 2018 Nov 28;13(11):e0206380. doi: 10.1371/journal.pone.0206380. eCollection 2018. PLoS One. 2018. PMID: 30485284 Free PMC article.
-
Performance of the MAGGIC heart failure risk score and its modification with the addition of discharge natriuretic peptides.ESC Heart Fail. 2018 Aug;5(4):610-619. doi: 10.1002/ehf2.12278. Epub 2018 Mar 9. ESC Heart Fail. 2018. PMID: 29520978 Free PMC article.
-
Performance of the Meta-Analysis Global Group in Chronic Heart Failure Score in Black Patients Compared With Whites.Circ Cardiovasc Qual Outcomes. 2019 Jul;12(7):e004714. doi: 10.1161/CIRCOUTCOMES.118.004714. Epub 2019 Jul 3. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31266369 Free PMC article.
-
Performance of current risk stratification models for predicting mortality in patients with heart failure: a systematic review and meta-analysis.Eur J Prev Cardiol. 2022 Nov 8;29(15):2027-2048. doi: 10.1093/eurjpc/zwac148. Eur J Prev Cardiol. 2022. PMID: 35919956
-
Biomarkers in heart failure: a focus on natriuretic peptides.Heart. 2024 May 10;110(11):809-818. doi: 10.1136/heartjnl-2020-318553. Heart. 2024. PMID: 37673654 Review.
Cited by
-
Suppression tumorigenicity 2 (ST2) turbidimetric immunoassay compared to enzyme-linked immunosorbent assay in predicting survival in heart failure patients with reduced ejection fraction.Clin Chim Acta. 2020 Nov;510:767-771. doi: 10.1016/j.cca.2020.08.039. Epub 2020 Sep 12. Clin Chim Acta. 2020. PMID: 32926842 Free PMC article.
-
Plasma Proteomic Profile Predicts Survival in Heart Failure With Reduced Ejection Fraction.Circ Genom Precis Med. 2021 Jun;14(3):e003140. doi: 10.1161/CIRCGEN.120.003140. Epub 2021 May 17. Circ Genom Precis Med. 2021. PMID: 33999650 Free PMC article. Clinical Trial.
-
Prognostic value of natriuretic peptides in heart failure: systematic review and meta-analysis.Heart Fail Rev. 2022 Mar;27(2):645-654. doi: 10.1007/s10741-021-10136-3. Epub 2021 Jul 5. Heart Fail Rev. 2022. PMID: 34227029
-
Validation of the Meta-Analysis Global Group in Chronic Heart Failure risk score for the prediction of 1-year mortality in a Chinese cohort.Chin Med J (Engl). 2022 Dec 5;135(23):2829-2835. doi: 10.1097/CM9.0000000000002026. Chin Med J (Engl). 2022. PMID: 36728514 Free PMC article.
-
Development and Validation of a Protein Risk Score for Mortality in Heart Failure : A Community Cohort Study.Ann Intern Med. 2024 Jan;177(1):39-49. doi: 10.7326/M23-2328. Epub 2024 Jan 2. Ann Intern Med. 2024. PMID: 38163367 Free PMC article.
References
-
- Lindenauer PK, Remus D, Roman S, Rothberg MB, Benjamin EM, Ma A, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007;356:486–96. - PubMed
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics−-2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Cleland JG, Chiswell K, Teerlink JR, Stevens S, Fiuzat M, Givertz MM, et al. Predictors of postdischarge outcomes from information acquired shortly after admission for acute heart failure: a report from the Placebo-Controlled Randomized Study of the Selective A1 Adenosine Receptor Antagonist Rolofylline for Patients Hospitalized With Acute Decompensated Heart Failure and Volume Overload to Assess Treatment Effect on Congestion and Renal Function (PROTECT) Study. Circulation Heart failure. 2014;7:76–87. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
