

Platelet Function Changes during Neonatal Cardiopulmonary Bypass Surgery: Mechanistic Basis and Lack of Correlation with Excessive Bleeding
- PMID: 31752040
- PMCID: PMC7003188
- DOI: 10.1055/s-0039-1700517
Platelet Function Changes during Neonatal Cardiopulmonary Bypass Surgery: Mechanistic Basis and Lack of Correlation with Excessive Bleeding
Abstract
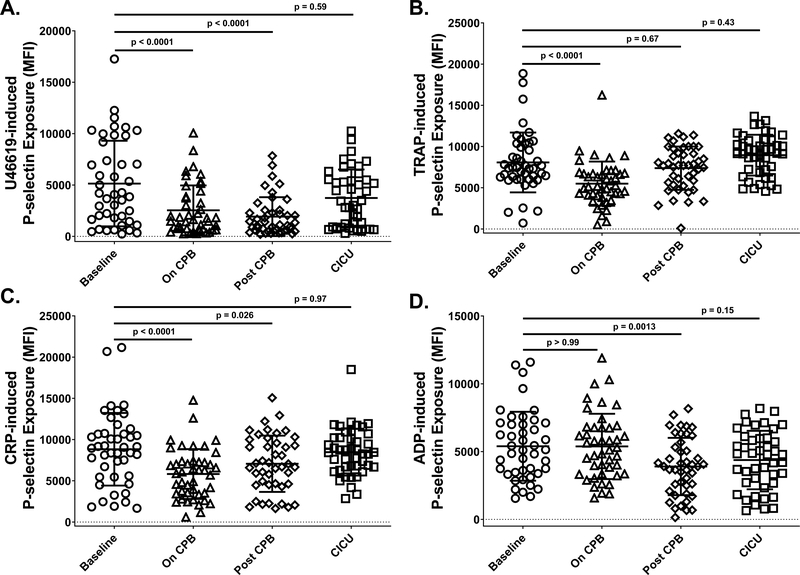
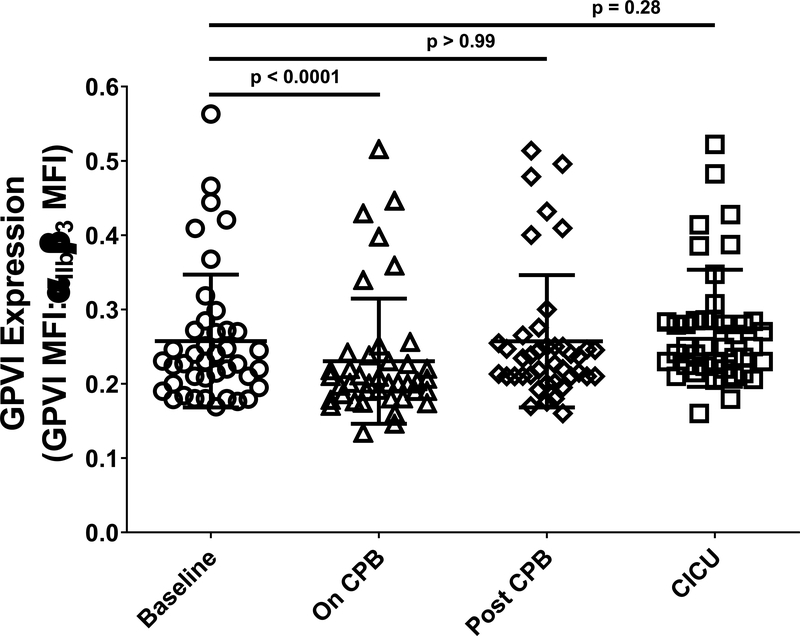
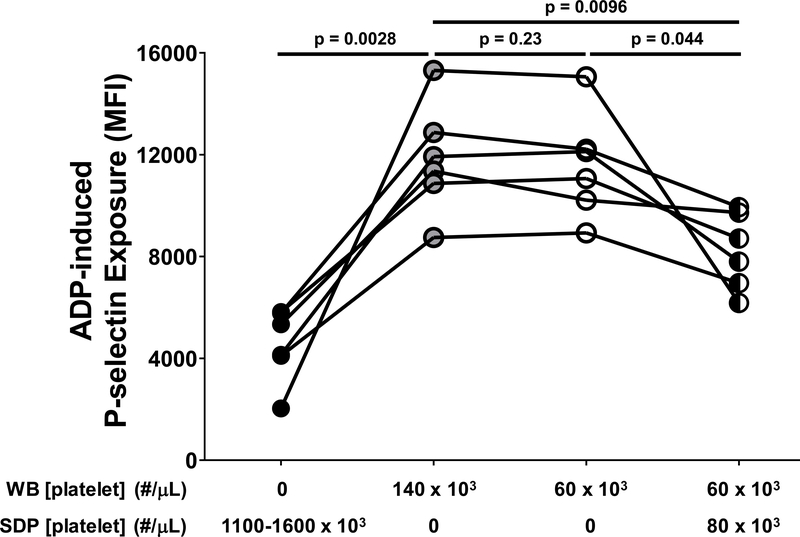
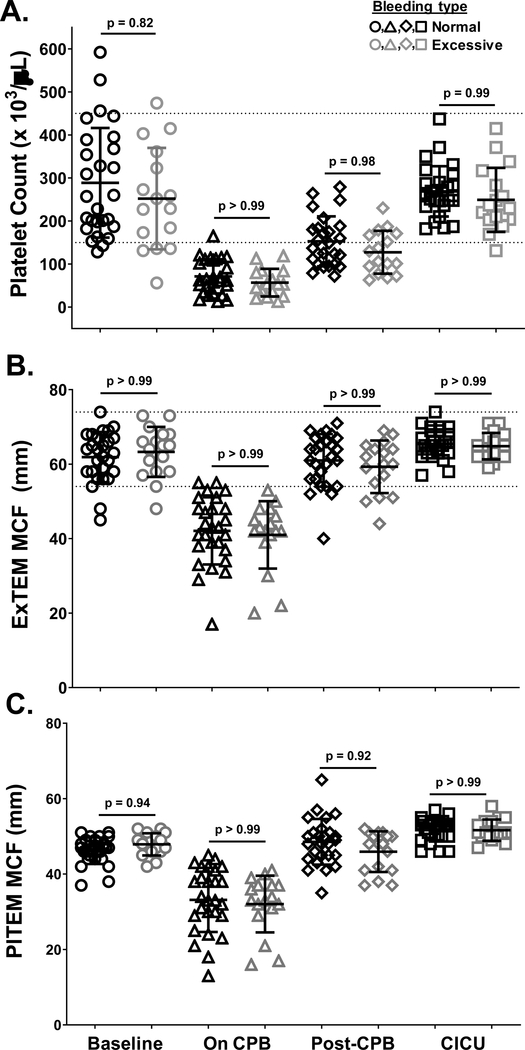
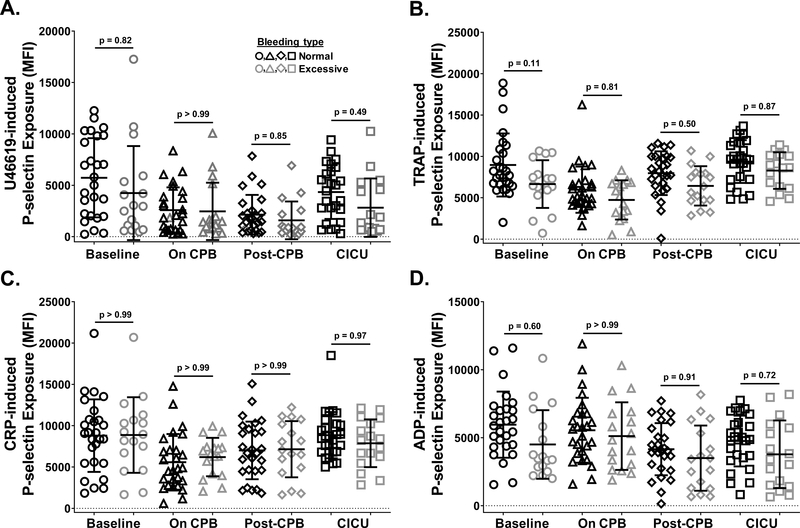
Thrombocytopenia and platelet dysfunction induced by extracorporeal blood circulation are thought to contribute to postsurgical bleeding complications in neonates undergoing cardiac surgery with cardiopulmonary bypass (CPB). In this study, we examined how changes in platelet function relate to changes in platelet count and to excessive bleeding in neonatal CPB surgery. Platelet counts and platelet P-selectin exposure in response to agonist stimulation were measured at four times before, during, and after CPB surgery in neonates with normal versus excessive levels of postsurgical bleeding. Relative to baseline, platelet counts were reduced in patients while on CPB, as was platelet activation by the thromboxane A2 analog U46619, thrombin receptor activating peptide (TRAP), and collagen-related peptide (CRP). Platelet activation by adenosine diphosphate (ADP) was instead reduced after platelet transfusion. We provide evidence that thrombocytopenia is a likely contributor to CPB-associated defects in platelet responsiveness to U46619 and TRAP, CPB-induced collagen receptor downregulation likely contributes to defective platelet responsiveness to CRP, and platelet transfusion may contribute to defective platelet responses to ADP. Platelet transfusion restored to baseline levels platelet counts and responsiveness to all agonists except ADP but did not prevent excessive bleeding in all patients. We conclude that platelet count and function defects are characteristic of neonatal CPB surgery and that platelet transfusion corrects these defects. However, since CPB-associated coagulopathy is multifactorial, platelet transfusion alone is insufficient to treat bleeding events in all patients. Therefore, platelet transfusion must be combined with treatment of other factors that contribute to the coagulopathy to prevent excessive bleeding.
Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
None declared.
Figures


References
-
- Manno CS, Hedberg KW, Kim HC, et al. Comparison of the hemostatic effects of fresh whole blood, stored whole blood, and components after open heart surgery in children. Blood 1991; 77(5): 930–936. - PubMed
-
- Petaja J, Lundstrom U, Leijala M, et al. Bleeding and use of blood products after heart operations in infants. J Thorac Cardiovasc Surg 1995; 109(3): 524–529. - PubMed
-
- Chambers LA, Cohen DM, Davis JT. Transfusion patterns in pediatric open heart surgery. Transfusion 1996; 36(2): 150–154. - PubMed
-
- Williams GD, Bratton SL, Riley EC, et al. Association between age and blood loss in children undergoing open heart operations. Ann Thorac Surg 1998; 66(3): 870–875; discussion 875–876. - PubMed
-
- Williams GD, Bratton SL, Ramamoorthy C. Factors associated with blood loss and blood product transfusions: a multivariate analysis in children after open-heart surgery. Anesth Analg 1999; 89(1): 57–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R35 HL139937/HL/NHLBI NIH HHS/United States
- U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute/T32 HL-07209
- U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute/R35 HL-139937
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
