

Evaluation of the Accuracy of Liquid-Based Oral Brush Cytology in Screening for Oral Squamous Cell Carcinoma
- PMID: 31752196
- PMCID: PMC6896118
- DOI: 10.3390/cancers11111813
Evaluation of the Accuracy of Liquid-Based Oral Brush Cytology in Screening for Oral Squamous Cell Carcinoma
Abstract
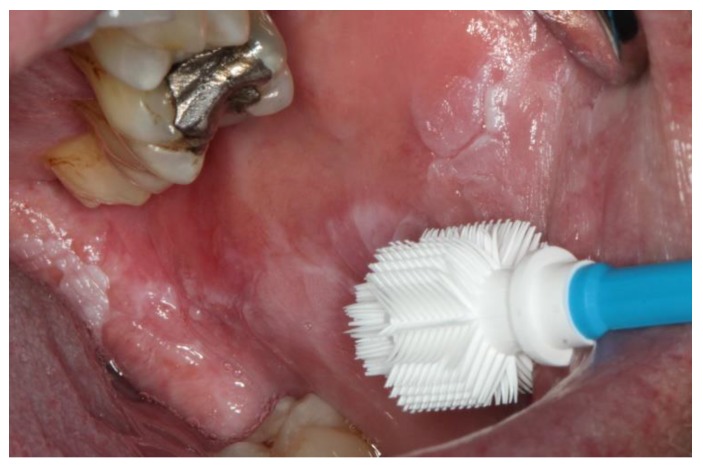
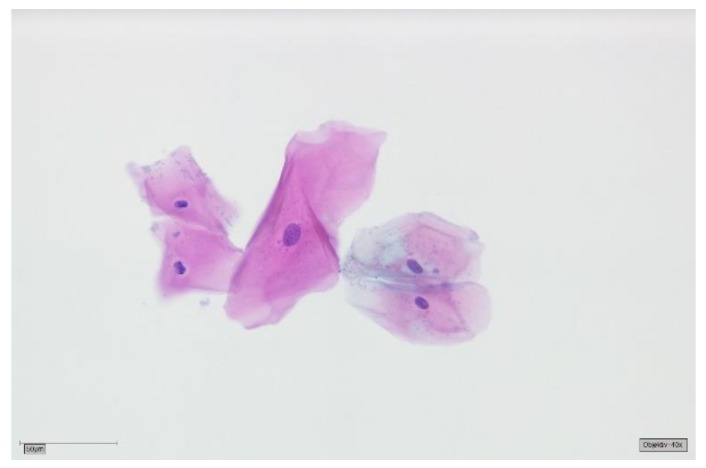
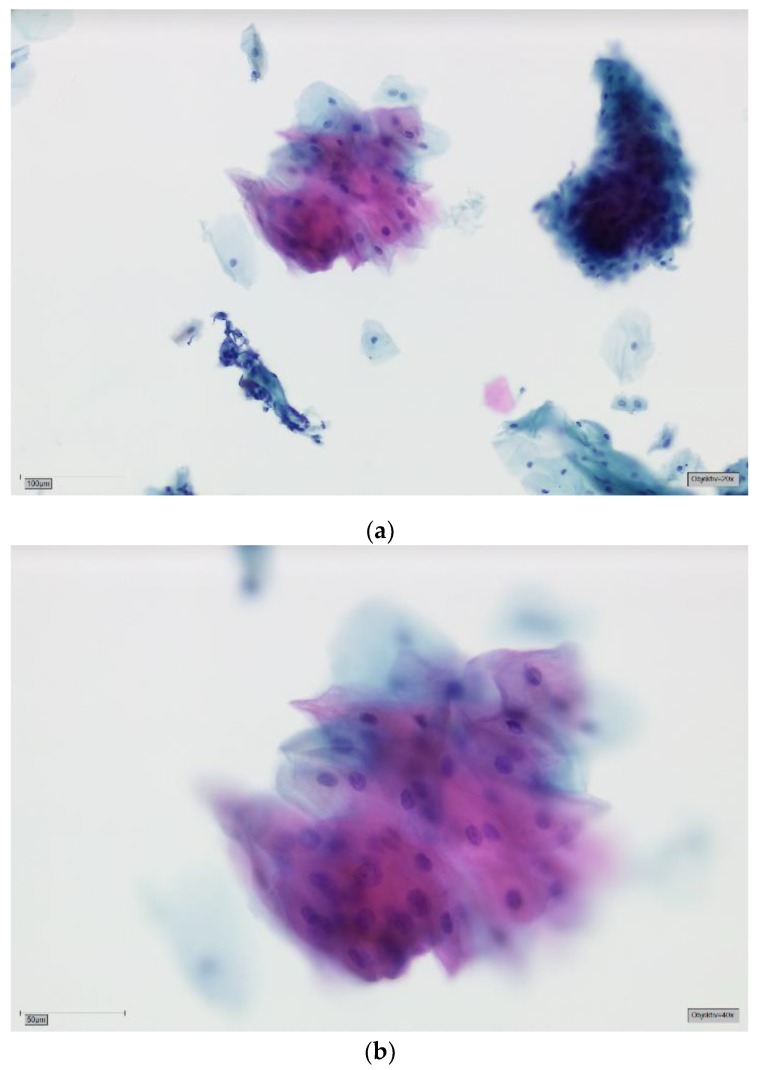
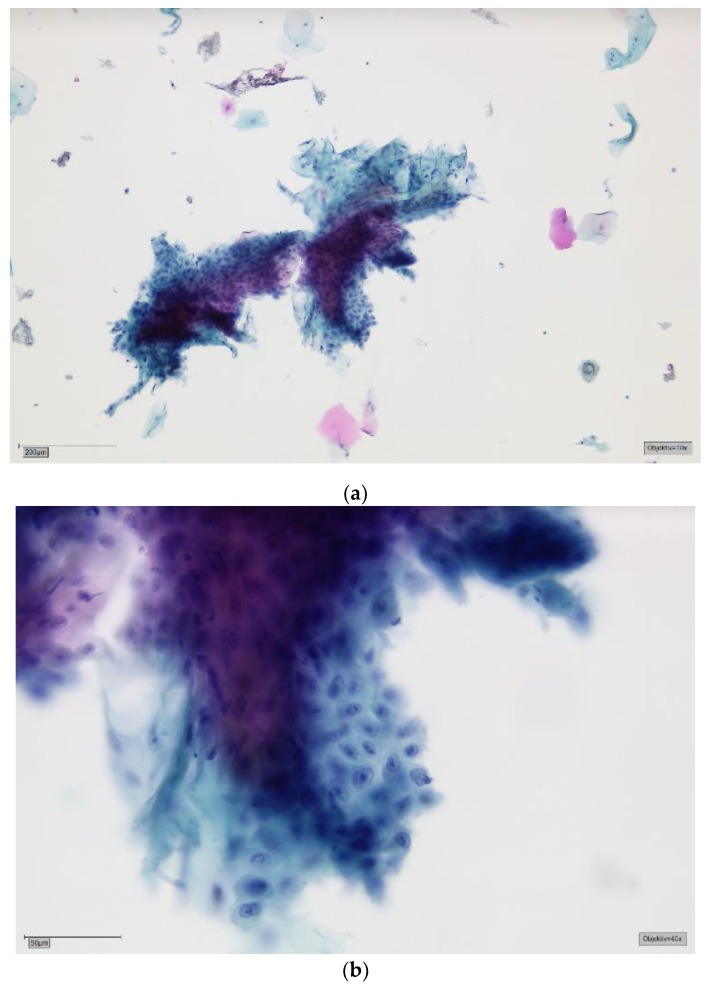
This study evaluates the accuracy of the results of liquid-based oral brush cytology and compares it to the histology and/or the clinical follow-ups of the respective patients. A total of 1352 exfoliated specimens were collected with an Orcellex brush from an identical number of oral lesions, then cytological diagnoses were made using liquid-based cytology. The final diagnoses in the study were 105 histologically proven squamous cell carcinomas (SCCs), 744 potentially malignant lesions and 503 cases of traumatic, inflammatory or benign hyperplastic oral lesions. The sensitivity and specificity of the liquid-based brush biopsy were 95.6% (95% CI 94.5-96.7%) and 84.9% (95% CI 83.0-86.8%), respectively. This led to the conclusion that brush biopsy is potentially a highly sensitive and reliable method to make cytological diagnoses of oral neoplasia. The main advantage of a brush biopsy over a scalpel biopsy is that it is less invasive and is more tolerated by the patients. Therefore, more lesions can be screened and more cancers can be detected at an early stage.
Keywords: brush biopsy; liquid-based cytology; oral cancer; squamous cell carcinoma.
Conflict of interest statement
Torsten W. Remmerbach is CEO of the German Association of Oral Diagnostics (DGOD mbH, Leipzig, Germany).
Figures
References
-
- Robert Koch-Institut . Krebs in Deutschland 2013/2014. Robert Koch-Institut; Berlin, Germany: 2014.
LinkOut - more resources
Full Text Sources
