

Analysis of key clinical features for achieving complete remission in stage III and IV non-small cell lung cancer patients
- PMID: 31752884
- PMCID: PMC6873580
- DOI: 10.1186/s12931-019-1235-3
Analysis of key clinical features for achieving complete remission in stage III and IV non-small cell lung cancer patients
Abstract
Background: Although development of immune checkpoint inhibitors and various molecular target agents has extended overall survival time (OS) in advanced non-small cell lung cancer (NSCLC), a complete cure remains rare. We aimed to identify features and treatment modalities of complete remission (CR) cases in stages III and IV NSCLC by analyzing long-term survivors whose OS exceeded 3 years.
Methods: From our hospital database, 1,699 patients, registered as lung cancer between 1st Mar 2004 and 30th Apr 2011, were retrospectively examined. Stage III or IV histologically or cytologically confirmed NSCLC patients with chemotherapy initiated during this period were enrolled. A Cox proportion hazards regression model was used. Data collection was closed on 13th Feb 2017.
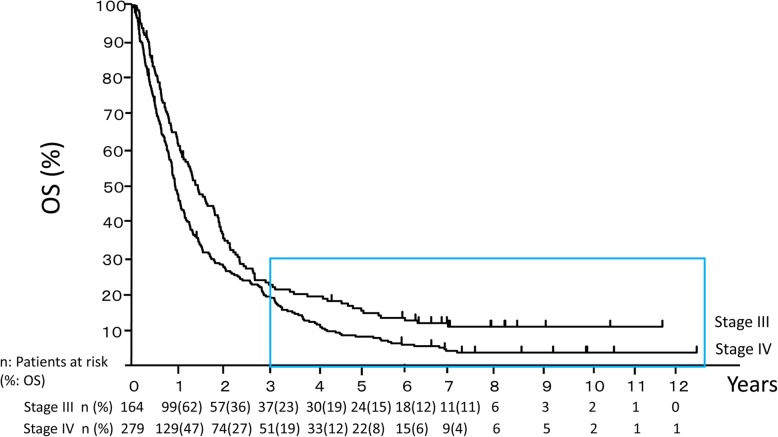
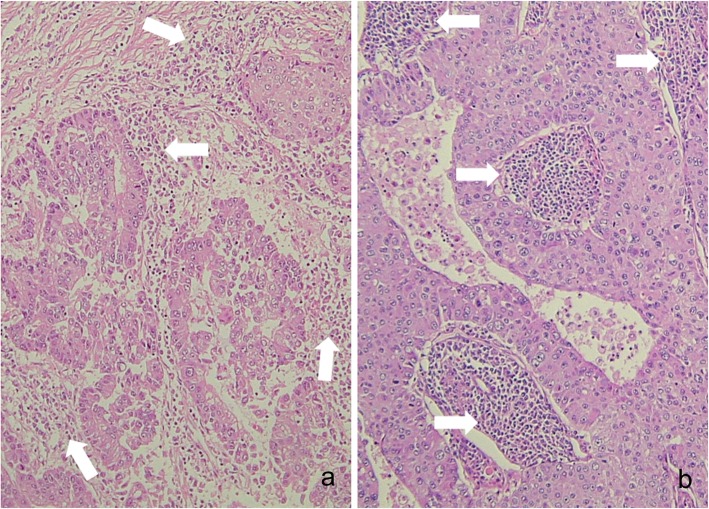
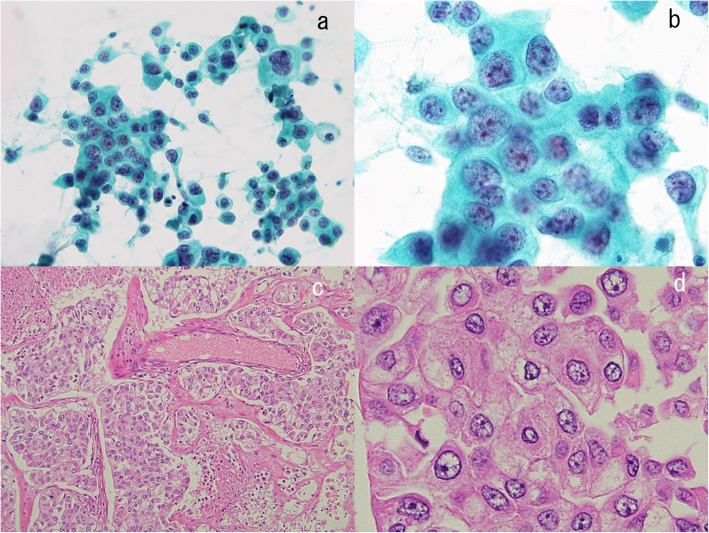
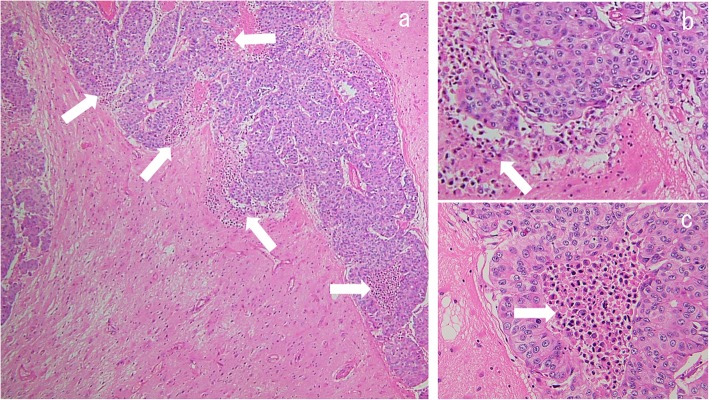
Results: There were 164 stage III and 279 stage IV patients, including 37 (22.6%) and 51 (18.3%) long-term survivors and 12 (7.3%) and 5 (1.8%) CR patients, respectively. The long-term survivors were divided into three groups: 3 ≤ OS < 5 years, 5 years ≤ OS with tumor, and 5 years ≤ OS without tumor (CR). The median OS of these groups were 1,405, 2,238, and 2,876 days in stage III and 1,368, 2,503, and 2,643 days in stage IV, respectively. The mean chemotherapy cycle numbers were 16, 20, and 10 in stage III and 24, 25, and 5 in stage IV, respectively. In the stage III CR group, all patients received chemoradiation, all oligometastases were controlled by radiation, and none had brain metastases. Compared with non-CR patients, the stage IV CR patients had smaller primary tumors and fewer metastases, which were independent prognostic factors for OS among long-term survivors. The 80% stage IV CR patients received radiation or surgery for controlling primary tumors, and the surgery rate for oligometastases was high. Pathological findings in the stage IV CR patients revealed that numerous inflammatory cells existed around and inside resected lung and brain tumors, indicating strong immune response.
Conclusions: Multiple line chemotherapies with primary and oligometastatic controls by surgery and/or radiation might achieve cure in certain advanced NSCLC. Cure strategies must be changed according to stage III or IV. This study was retrospectively registered on 16th Jun 2019 in UMIN Clinical Trials Registry (number UMIN000037078).
Keywords: advanced non-small cell lung cancer; complete remission; oligometastases; radiation; surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Ohe Y, Ohashi Y, Kubota K, Tamura T, Nakagawa K, Negoro S, Nishiwaki Y, Saijo N, Ariyoshi Y, Fukuoka M. Randomized phase III study of cisplatin plus irinotecan versus carboplatin plus paclitaxel, cisplatin plus gemcitabine, and cisplatin plus vinorelbine for advanced non-small-cell lung cancer: Four-Arm Cooperative Study in Japan. Ann Oncol. 2007;18:317–323. doi: 10.1093/annonc/mdl377. - DOI - PubMed
-
- Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. doi: 10.1056/NEJMoa040938. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
