

Respective contribution of intensive care unit-acquired limb muscle and severe diaphragm weakness on weaning outcome and mortality: a post hoc analysis of two cohorts
- PMID: 31752937
- PMCID: PMC6873450
- DOI: 10.1186/s13054-019-2650-z
Respective contribution of intensive care unit-acquired limb muscle and severe diaphragm weakness on weaning outcome and mortality: a post hoc analysis of two cohorts
Abstract
Background: Intensive care unit (ICU)-acquired weakness (ICU-AW) and ICU-acquired diaphragm dysfunction (ICU-DD) occur frequently in mechanically ventilated (MV) patients. It is unknown whether they have different risk factors and different impacts on outcome. This study was designed to (1) describe the respective risk factors associated with ICU-AW and severe ICU-DD and (2) evaluate the respective impact of ICU-AW and severe ICU-DD on outcome.
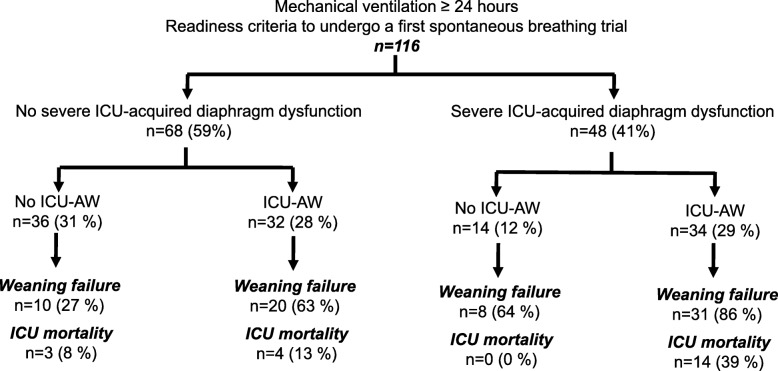
Methods: Post hoc analysis of two prospective cohort studies conducted in two ICUs. In patients mechanically ventilated for at least 24 h undergoing a first spontaneous breathing trial, severe ICU-DD was defined as diaphragm twitch pressure < 7 cmH2O and ICU-AW was defined as Medical Research Council Score < 48.
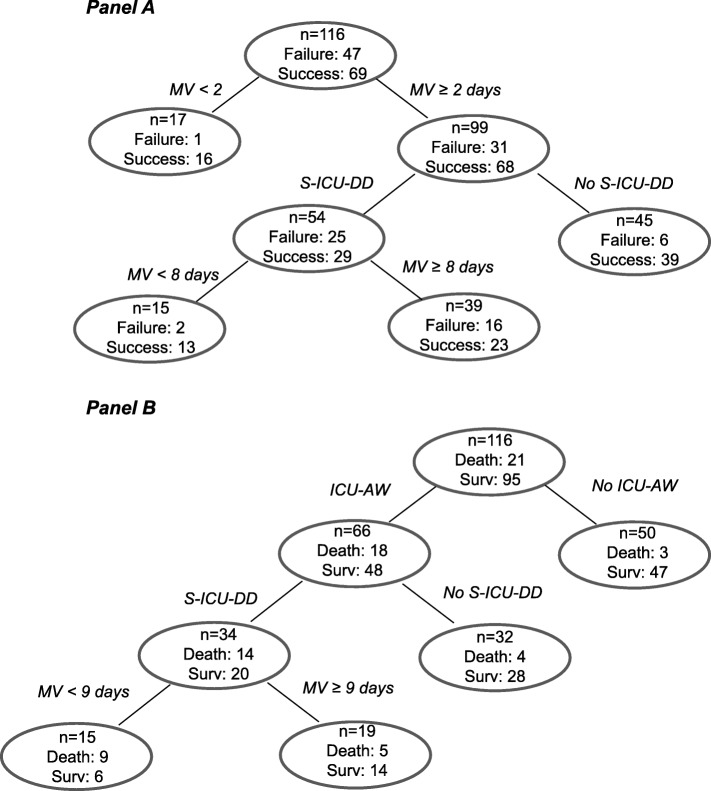
Results: One hundred sixteen patients were assessed. Factors independently associated with severe ICU-DD were age, longer duration of MV, and exposure to sufentanil, and those factors associated with ICU-AW were longer duration of MV and exposure to norepinephrine. Severe ICU-DD (OR 3.56, p = 0.008), but not ICU-AW, was independently associated with weaning failure (59%). ICU-AW (OR 4.30, p = 0.033), but not severe ICU-DD, was associated with ICU mortality. Weaning failure and mortality rate were higher in patients with both severe ICU-DD and ICU-AW (86% and 39%, respectively) than in patients with either severe ICU-DD (64% and 0%) or ICU-AW (63% and 13%).
Conclusion: Severe ICU-DD and ICU-AW have different risk factors and different impacts on weaning failure and mortality. The impact of the combination of ICU-DD and ICU-AW is more pronounced than their individual impact.
Keywords: Diaphragm; Intensive care unit; Magnetic stimulation; Mechanical ventilation; Muscles; Weakness; Weaning.
Conflict of interest statement
Martin Dres reports personal fees from Lungpacer, outside the submitted work. Boris Jung declares no competing interests. Nicolas Molinari declares no competing interests. Federico Manna declares no competing interests. Gerald Chanques reports personal fees from Aspen medical and personal fees from Orion pharma, during the conduct of the study. Samir Jaber declares no competing interests. Thomas Similowski reports receiving personal fees from Almirall France, personal fees from AstraZeneca France, corporate personal fees from Boehringer Ingelheim France, personal fees from GlaxoSmithKline France, personal fees from Invacare, personal fees from Mundipharma, personal fees and nonfinancial support from Novartis France, personal fees from Pfizer France, grants and personal fees from Pierre Fabre Médicaments, personal fees from Takeda, personal fees from Teva Pharma, and personal fees from Lungpacer Medical Inc., all outside the submitted work. Alexandre Demoule reports personal fees from Medtronic; grants, personal fees, and non-financial support from Philips; personal fees from Baxter; personal fees from Hamilton; personal fees and non-financial support from Fisher & Paykel; grants from French Ministry of Health; personal fees from Getinge; grants and personal fees from Respinor; and grants and non-financial support from Lungpacer. Brunop-Pierre Dubé received personal fees from Grifols, Boehringer Ingelheim and Roche, and has signed clinical research contracts with Sanofi, Roche and Boehringer Ingelheim.
Figures
References
-
- Demoule A, Jung B, Prodanovic H, Molinari N, Chanques G, Coirault C, et al. Diaphragm dysfunction on admission to the intensive care unit. Prevalence, risk factors, and prognostic impact-a prospective study. Am J Respir Crit Care Med. 2013;188:213–219. doi: 10.1164/rccm.201209-1668OC. - DOI - PubMed
-
- Dres M, Dubé B-P, Mayaux J, Delemazure J, Reuter D, Brochard L, et al. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med. 2017;195:57–66. doi: 10.1164/rccm.201602-0367OC. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- 2005 Programme Hospitalier de Recherche Clinique (PHRC)/French Ministry of Health/International
- bourse de mobilité 2015/Société de Réanimation de Langue Française/International
- Short Term Fellowship program/European Respiratory Society/International
- 2015 Bernhard Dräger Award/European Society of Intensive Care Medicine/International
- FDM 20150734498/Fondation pour la Recherche Médicale/International
LinkOut - more resources
Full Text Sources
Medical
