

Effects of inspiratory flow on lung stress, pendelluft, and ventilation heterogeneity in ARDS: a physiological study
- PMID: 31752952
- PMCID: PMC6873770
- DOI: 10.1186/s13054-019-2641-0
Effects of inspiratory flow on lung stress, pendelluft, and ventilation heterogeneity in ARDS: a physiological study
Abstract
Background: High inspiratory flow might damage the lungs by mechanisms not fully understood yet. We hypothesized that increasing inspiratory flow would increase lung stress, ventilation heterogeneity, and pendelluft in ARDS patients undergoing volume-controlled ventilation with constant tidal volume and that higher PEEP levels would reduce this phenomenon.
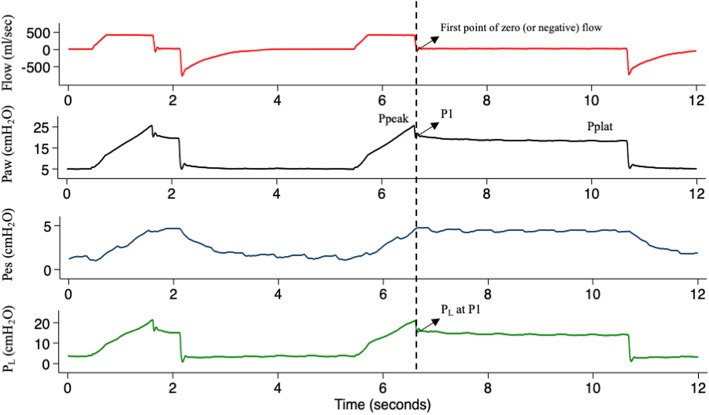
Methods: Ten ARDS patients were studied during protective volume-controlled ventilation. Three inspiratory flows (400, 800, and 1200 ml/s) and two PEEP levels (5 and 15 cmH2O) were applied in random order to each patient. Airway and esophageal pressures were recorded, end-inspiratory and end-expiratory holds were performed, and ventilation distribution was measured with electrical impedance tomography. Peak and plateau airway and transpulmonary pressures were recorded, together with the airway and transpulmonary pressure corresponding to the first point of zero end-inspiratory flow (P1). Ventilation heterogeneity was measured by the EIT-based global inhomogeneity (GI) index. Pendelluft was measured as the absolute difference between pixel-level inflation measured at plateau pressure minus P1.
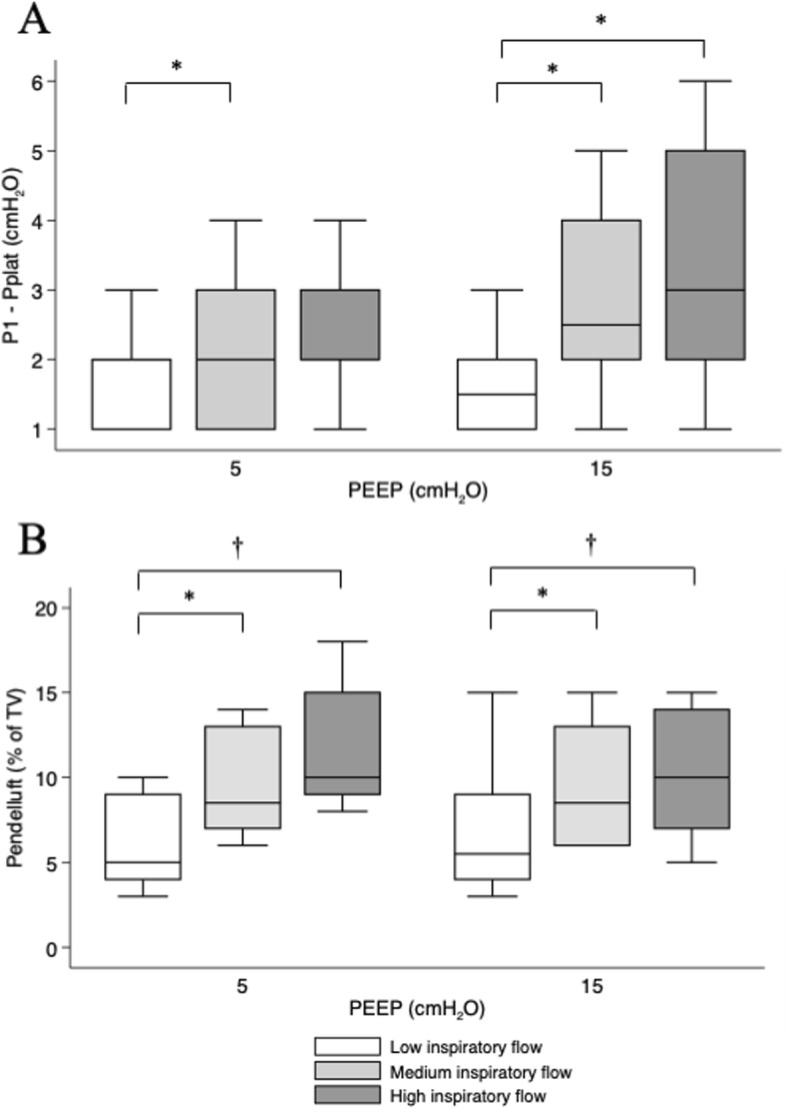
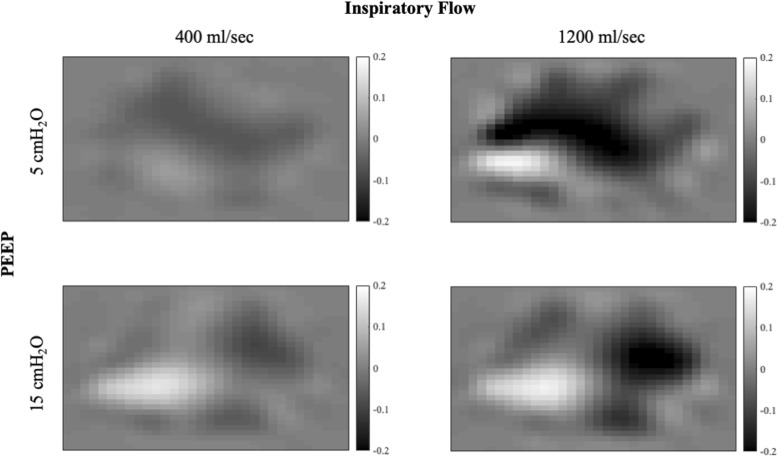
Results: Plateau airway and transpulmonary pressure was not affected by inspiratory flow, while P1 increased at increasing inspiratory flow. The difference between P1 and plateau pressure was higher at higher flows at both PEEP levels (p < 0.001). While higher PEEP reduced heterogeneity of ventilation, higher inspiratory flow increased GI (p = 0.05), irrespective of the PEEP level. Finally, gas volume undergoing pendelluft was larger at higher inspiratory flow (p < 0.001), while PEEP had no effect.
Conclusions: The present exploratory analysis suggests that higher inspiratory flow increases additional inspiratory pressure, heterogeneity of ventilation, and pendelluft while PEEP has negligible effects on these flow-dependent phenomena. The clinical significance of these findings needs to be further clarified.
Keywords: ARDS; Electrical impedance tomography; Heterogeneity; Inspiratory flow.
Conflict of interest statement
AP reports personal fees from Xenios, Maquet, and Baxter, outside the submitted work. TM reports personal fees from Drager, outside the submitted work. The other authors declare that they have no competing interests.
Figures
References
-
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
