

Outcomes of Stenotrophomonas maltophilia hospital-acquired pneumonia in intensive care unit: a nationwide retrospective study
- PMID: 31752976
- PMCID: PMC6873544
- DOI: 10.1186/s13054-019-2649-5
Outcomes of Stenotrophomonas maltophilia hospital-acquired pneumonia in intensive care unit: a nationwide retrospective study
Abstract
Background: There is little descriptive data on Stenotrophomonas maltophilia hospital-acquired pneumonia (HAP) in critically ill patients. The optimal modalities of antimicrobial therapy remain to be determined. Our objective was to describe the epidemiology and prognostic factors associated with S. maltophilia pneumonia, focusing on antimicrobial therapy.
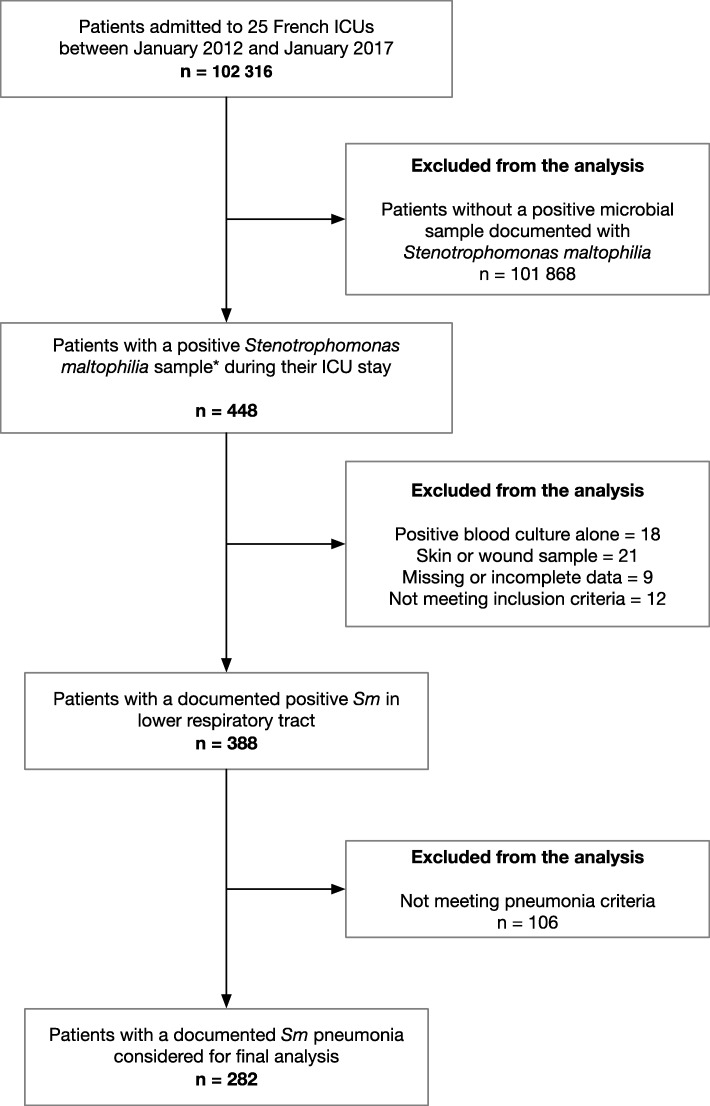
Methods: This nationwide retrospective study included all patients admitted to 25 French mixed intensive care units between 2012 and 2017 with hospital-acquired S. maltophilia HAP during intensive care unit stay. Primary endpoint was time to in-hospital death. Secondary endpoints included microbiologic effectiveness and antimicrobial therapeutic modalities such as delay to appropriate antimicrobial treatment, mono versus combination therapy, and duration of antimicrobial therapy.
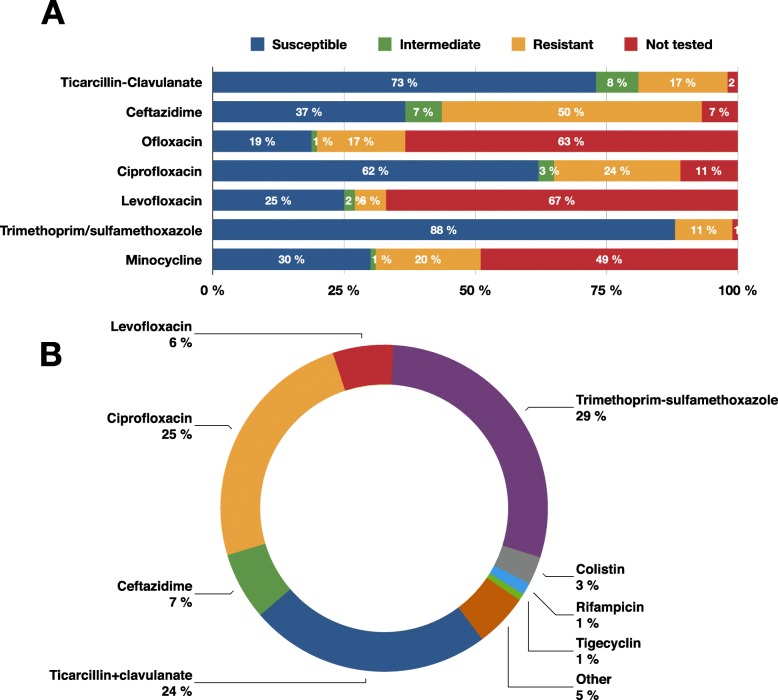
Results: Of the 282 patients included, 84% were intubated at S. maltophilia HAP diagnosis for duration of 11 [5-18] days. The Simplified Acute Physiology Score II was 47 [36-63], and the in-hospital mortality was 49.7%. Underlying chronic pulmonary comorbidities were present in 14.1% of cases. Empirical antimicrobial therapy was considered effective on S. maltophilia according to susceptibility patterns in only 30% of cases. Delay to appropriate antimicrobial treatment had, however, no significant impact on the primary endpoint. Survival analysis did not show any benefit from combination antimicrobial therapy (HR = 1.27, 95%CI [0.88; 1.83], p = 0.20) or prolonged antimicrobial therapy for more than 7 days (HR = 1.06, 95%CI [0.6; 1.86], p = 0.84). No differences were noted in in-hospital death irrespective of an appropriate and timely empiric antimicrobial therapy between mono- versus polymicrobial S. maltophilia HAP (p = 0.273). The duration of ventilation prior to S. maltophilia HAP diagnosis and ICU length of stay were shorter in patients with monomicrobial S. maltophilia HAP (p = 0.031 and p = 0.034 respectively).
Conclusions: S. maltophilia HAP occurred in severe, long-stay intensive care patients who mainly required prolonged invasive ventilation. Empirical antimicrobial therapy was barely effective while antimicrobial treatment modalities had no significant impact on hospital survival.
Trial registration: clinicaltrials.gov, NCT03506191.
Keywords: Antimicrobial therapy; Combination therapy; Hospital-acquired pneumonia; Intensive care; Stenotrophomonas maltophilia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Healthcare-associated infections in intensive care units - Annual Epidemiological Report for 2015. European Centre for Disease Prevention and Control. 2017. Available from: http://ecdc.europa.eu/en/publications-data/healthcare-associated-infecti.... [cited 2018 Aug 27]
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
