

Immune checkpoint inhibitor related myasthenia gravis: single center experience and systematic review of the literature
- PMID: 31753014
- PMCID: PMC6868691
- DOI: 10.1186/s40425-019-0774-y
Immune checkpoint inhibitor related myasthenia gravis: single center experience and systematic review of the literature
Abstract
Background: Myasthenia gravis (MG) is a rare but life-threatening adverse event of immune checkpoint inhibitors (ICI). Given the limited evidence, data from a large cohort of patients is needed to aid in recognition and management of this fatal complication.
Methods: We reviewed our institutional databases to identify patients who had cancer and MG in the setting of ICI. We systematically reviewed the literature through August 2018 to identify all similar reported patients. We collected data on clinical and diagnostic features, management, and outcomes of these cases.
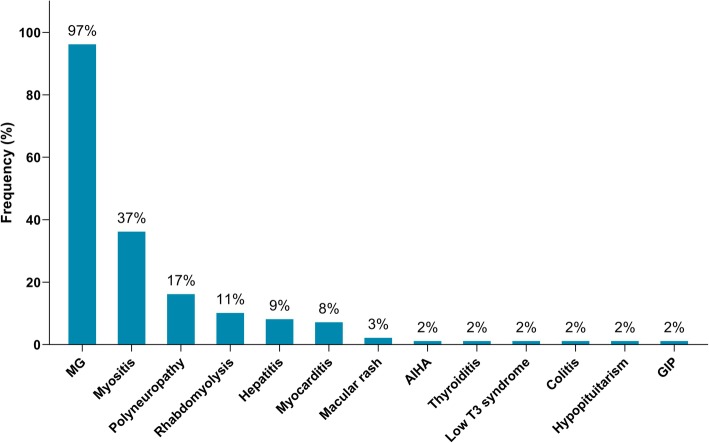
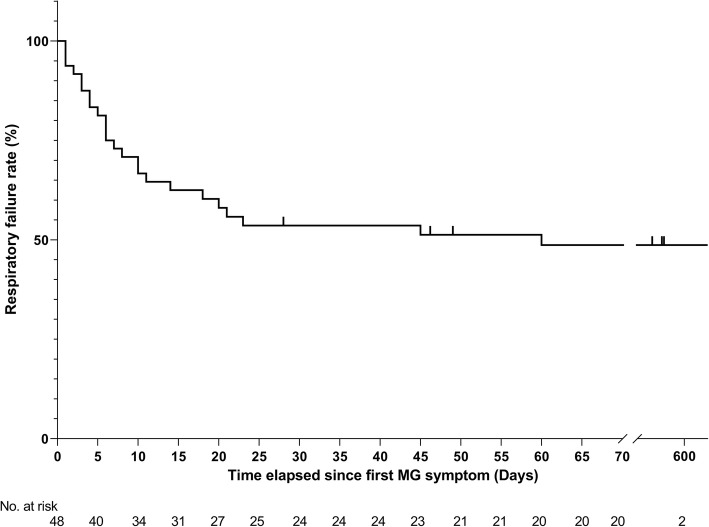
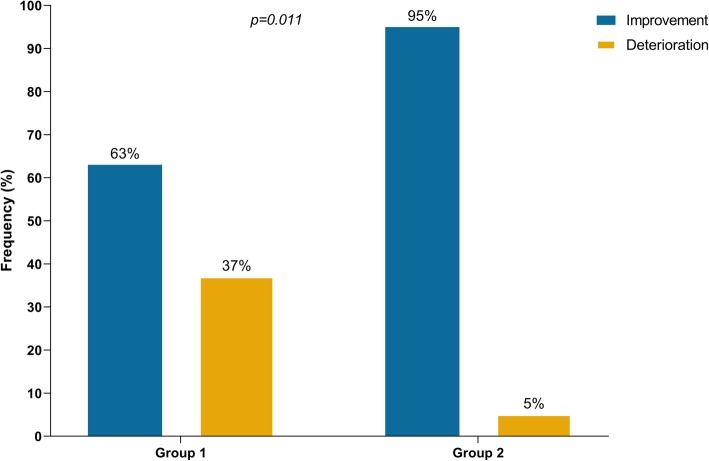
Results: Sixty-five patients were identified. Median age was 73 years; 42 (65%) were males, 31 (48%) had metastatic melanoma, and 13 (20%) had a preexisting MG before ICI initiation. Most patients received anti-PD-1 (82%). Sixty-three patients (97%) developed ICI-related MG (new onset or disease flare) after a median of 4 weeks (1 to 16 weeks) of ICI initiation. Twenty-four patients (37%) experienced concurrent myositis, and respiratory failure occurred in 29 (45%). ICI was discontinued in 61 patients (97%). Death was reported in 24 patients (38%); 15 (23%) due to MG complication. A better outcome was observed in patients who received intravenous immunoglobulin (IVIG) or plasmapheresis (PLEX) as first-line therapy than in those who received steroids alone (95% vs 63% improvement of MG symptoms, p = 0.011).
Conclusions: MG is a life-threatening adverse event of acute onset and rapid progression after ICI initiation. Early use of IVIG or PLEX, regardless of initial symptoms severity, may lead to better outcomes than steroids alone. Our data suggest the need to reassess the current recommendations for management of ICI-related MG until prospective longitudinal studies are conducted to establish the ideal management approach for these patients.
Keywords: Immune checkpoint inhibitors; Immunotherapy; Ipilimumab; Myasthenia gravis; Nivolumab; Pembrolizumab.
Conflict of interest statement
The authors declare that they have no competing interests
Figures

References
-
- Opdivo-nivolumab [package insert] Princeton NBMS. 2019.
-
- YERVOY-ipilimumab [package insert] Princeton NBS. 2019.
-
- KEYTRUDA- Pembrolizumab [package insert] County Cork IM. 2019.
-
- Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD, Schmidt H, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16(5):522–530. doi: 10.1016/S1470-2045(15)70122-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical