

Cone beam CT for perioperative imaging in hearing preservation Cochlear implantation - a human cadaveric study
- PMID: 31753027
- PMCID: PMC6873551
- DOI: 10.1186/s40463-019-0388-x
Cone beam CT for perioperative imaging in hearing preservation Cochlear implantation - a human cadaveric study
Abstract
Background: Knowledge of the cochlear implant array's precise position is important because of the correlation between electrode position and speech understanding. Several groups have provided recent image processing evidence to determine scalar translocation, angular insertion depth, and cochlear duct length (CDL); all of which are being used for patient-specific programming. Cone beam computed tomography (CBCT) is increasingly used in otology due to its superior resolution and low radiation dose. Our objectives are as followed: 1.Validate CBCT by measuring cochlear metrics, including basal turn diameter (A-value) and lateral wall cochlear duct length at different angular intervals and comparing it against microcomputed CT (uCT).2.Explore the relationship between measured lateral wall cochlear duct length at different angular intervals and insertion depth among 3 different length electrodes using CBCT.
Methods: The study was performed using fixed human cadaveric temporal bones in a tertiary academic centre. Ten temporal bones were subjected to the standard facial recess approach for cochlear implantation and imaged by CBCT followed by uCT. Measurements were performed on a three-dimensional reconstructed model of the cochlea. Sequential insertion of 3 electrodes (Med-El Flex24, 28 and Soft) was then performed in 5 bones and reimaged by CBCT. Statistical analysis was performed using Pearson's correlation.
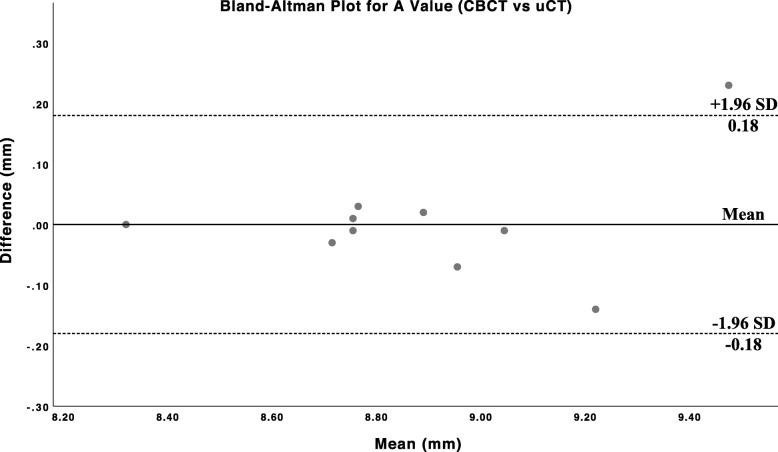
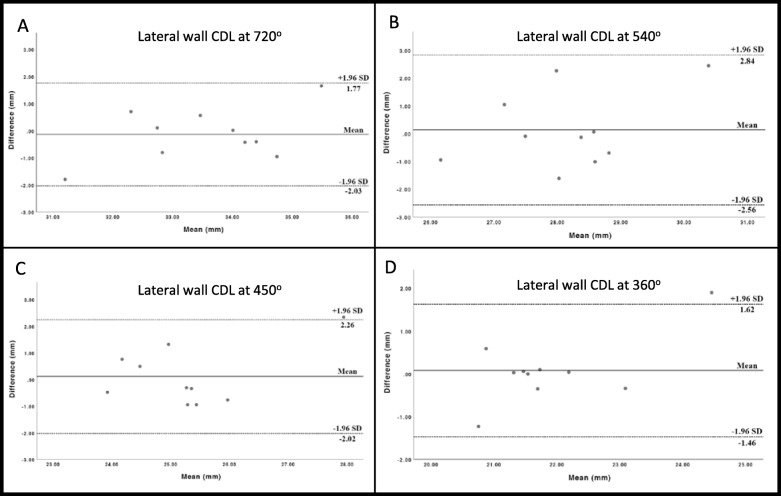
Results: There was good agreement between CBCT and uCT for cochlear metrics, validating the precision of CBCT against the current gold standard uCT in imaging. The A-value recorded by both modalities showed a high degree of linear correlation and did not differ by more than 0.23 mm in absolute values. For the measurement of lateral wall CDL at various points along the cochlea, there was a good correlation between both modalities at 360 deg and 720 deg (r = 0.85, p < 0.01 and r = 0.79, p < 0.01). The Flex24 electrode displayed consistent insertion depth across different bones.
Conclusions: CBCT reliably performs cochlear metrics and measures electrode insertion depth. The low radiation dose, fast acquisition time, diminished metallic artifacts and portability of CBCT make it a valid option for imaging in cochlear implant surgery.
Conflict of interest statement
None.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
