

Development and Validation of a Prediction Model for Atrial Fibrillation Using Electronic Health Records
- PMID: 31753441
- PMCID: PMC6884135
- DOI: 10.1016/j.jacep.2019.07.016
Development and Validation of a Prediction Model for Atrial Fibrillation Using Electronic Health Records
Abstract
Objectives: This study sought to determine whether the risk of atrial fibrillation AF can be estimated accurately by using routinely ascertained features in the electronic health record (EHR) and whether AF risk is associated with stroke.
Background: Early diagnosis of AF and treatment with anticoagulation may prevent strokes.
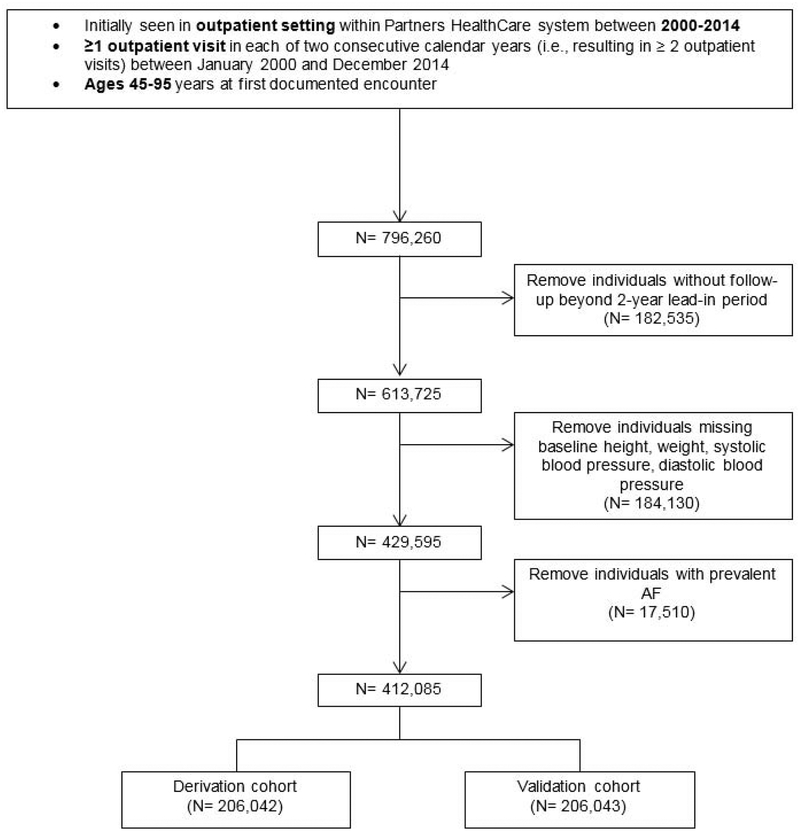
Methods: Using a multi-institutional EHR, this study identified 412,085 individuals 45 to 95 years of age without prevalent AF between 2000 and 2014. A prediction model was derived and validated for 5-year AF risk by using split-sample validation and model performance was compared with other methods of AF risk assessment.
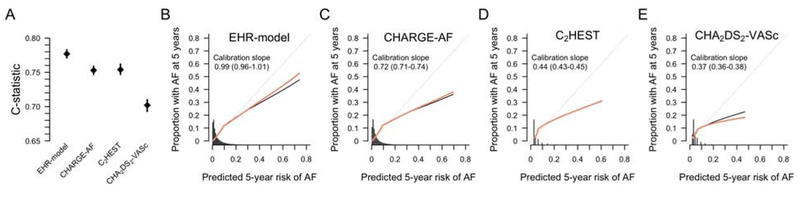
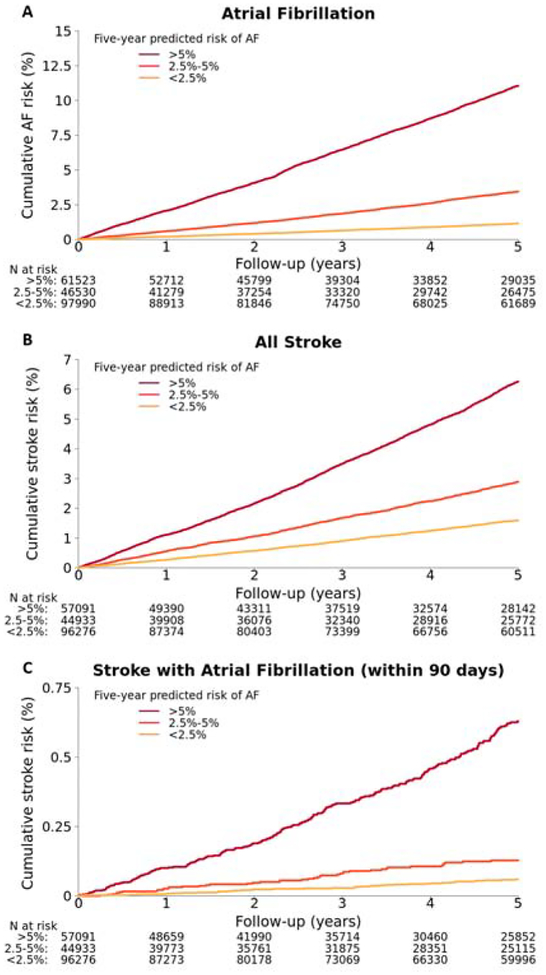
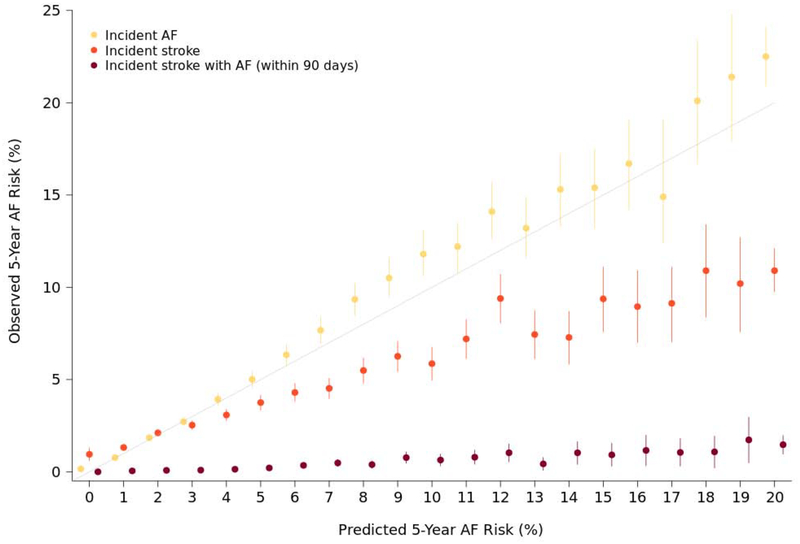
Results: Within 5 years, 14,334 individuals developed AF. In the derivation sample (7,216 AF events of 206,042 total), the optimal risk model included sex, age, race, smoking, height, weight, diastolic blood pressure, hypertension, hyperlipidemia, heart failure, coronary heart disease, valvular disease, prior stroke, peripheral arterial disease, chronic kidney disease, hypothyroidism, and quadratic terms for height, weight, and age. In the validation sample (7,118 AF events of 206,043 total) the AF risk model demonstrated good discrimination (C-statistic: 0.777; 95% confidence interval [CI:] 0.771 to 0.783) and calibration (0.99; 95% CI: 0.96 to 1.01). Model discrimination and calibration were superior to CHARGE-AF (Cohorts for Heart and Aging Research in Genomic Epidemiology AF) (C-statistic: 0.753; 95% CI: 0.747 to 0.759; calibration slope: 0.72; 95% CI: 0.71 to 0.74), C2HEST (Coronary artery disease / chronic obstructive pulmonary disease; Hypertension; Elderly [age ≥75 years]; Systolic heart failure; Thyroid disease [hyperthyroidism]) (C-statistic: 0.754; 95% CI: 0.747 to 0.762; calibration slope: 0.44; 95% CI: 0.43 to 0.45), and CHA2DS2-VASc (Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Prior stroke, transient ischemic attack [TIA], or thromboembolism, Vascular disease, Age 65-74 years, Sex category [female]) scores (C-statistic: 0.702; 95% CI: 0.693 to 0.710; calibration slope: 0.37; 95% CI: 0.36 to 0.38). AF risk discriminated incident stroke (n = 4,814; C-statistic: 0.684; 95% CI: 0.677 to 0.692) and stroke within 90 days of incident AF (n = 327; C-statistic: 0.789; 95% CI: 0.764 to 0.814).
Conclusions: A model developed from a real-world EHR database predicted AF accurately and stratified stroke risk. Incorporating AF prediction into EHRs may enable risk-guided screening for AF.
Keywords: atrial fibrillation; electronic health record; risk prediction; stroke.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Pre-Screening for Atrial Fibrillation Using the Electronic Health Record.JACC Clin Electrophysiol. 2019 Nov;5(11):1342-1343. doi: 10.1016/j.jacep.2019.08.019. JACC Clin Electrophysiol. 2019. PMID: 31753442 No abstract available.
References
-
- Miyasaka Y, Barnes ME, Gersh BJ et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–8. - PubMed
-
- Petty GW, Brown RD Jr., Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Ischemic stroke subtypes : a population-based study of functional outcome, survival, and recurrence. Stroke 2000;31:1062–8. - PubMed
-
- Lamassa M, Di Carlo A, Pracucci G et al. Characteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational hospital-based registry (The European Community Stroke Project). Stroke 2001;32:392–8. - PubMed
-
- Marini C, De Santis F, Sacco S et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005;36:1115–9. - PubMed
Publication types
MeSH terms
Grants and funding
- P50 HL120163/HL/NHLBI NIH HHS/United States
- R01 HL139731/HL/NHLBI NIH HHS/United States
- K23 NS086873/NS/NINDS NIH HHS/United States
- K24 HL105780/HL/NHLBI NIH HHS/United States
- R01 HL104156/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- T32 HL007208/HL/NHLBI NIH HHS/United States
- R01 NS103924/NS/NINDS NIH HHS/United States
- 2017039/DDCF/Doris Duke Charitable Foundation/United States
- 2016077/DDCF/Doris Duke Charitable Foundation/United States
- U54 HL120163/HL/NHLBI NIH HHS/United States
- R01 HL128914/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
