

Pro-inflammatory monocyte profile in patients with major depressive disorder and suicide behaviour and how ketamine induces anti-inflammatory M2 macrophages by NMDAR and mTOR
- PMID: 31753725
- PMCID: PMC6921226
- DOI: 10.1016/j.ebiom.2019.10.063
Pro-inflammatory monocyte profile in patients with major depressive disorder and suicide behaviour and how ketamine induces anti-inflammatory M2 macrophages by NMDAR and mTOR
Abstract
Background: Depression is a highly prevalent disorder that is one of the leading causes of disability worldwide. Despite an unknown aetiology, evidence suggests that the innate and adaptive immune systems play a significant role in the development and maintenance of major depressive disorder (MDD). The non-competitive glutamatergic N-methyl-D-aspartate receptor (NMDAR) antagonist, (R,S)-ketamine (ketamine), has demonstrated rapid and robust efficacy as an antidepressant when administered at sub-anaesthetic doses.
Methods: Our goal was to characterize the pro-inflammatory profile of patients with MDD by measuring pro-inflammatory cytokines in plasma and circulating monocyte subsets and to understand how ketamine induces an anti-inflammatory program in monocyte and macrophages in vitro and vivo.
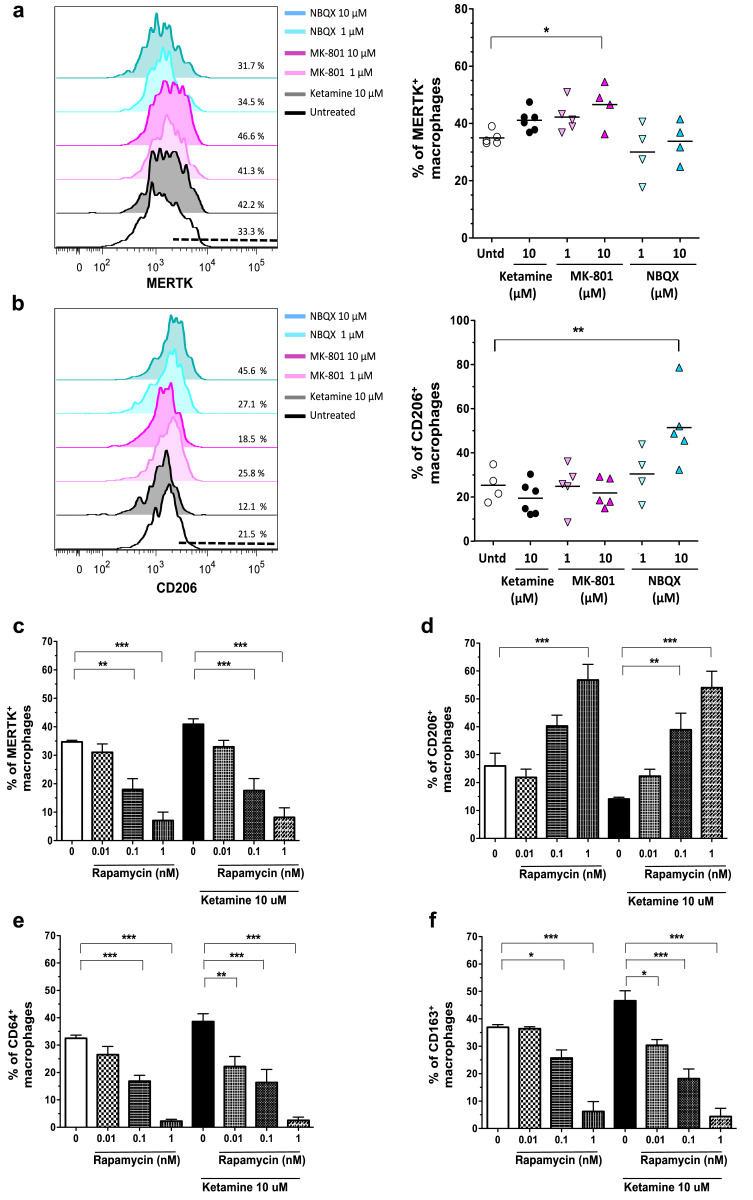
Finding: Our results show that patients with MDD without other comorbidities (N = 33) exhibited significantly higher levels of pro-inflammatory IL-12 and IL-6 in plasma and that these cytokines were associated with increased numbers of non-classical (CD11b+CD16brightCD14neg) monocytes and increased activation state (CD40+CD86+) of classical monocytes in circulation. Remarkably, we have demonstrated that sub-anaesthetic doses of ketamine programs human monocytes into M2c-like macrophages by inducing high levels of CD163 and MERTK with intermediate levels of CD64 and stimulating mTOR-associated gene expression in vitro. The NMDAR antagonist MK-801, but not the α-amino-3‑hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR) antagonist, NBQX, also polarizes macrophages to an M2c-like phenotype, but this phenotype disappears upon mTOR pathway inhibition. Sub-anaesthetic doses (10 mg/kg) of ketamine administration in mice both promote reduction of circulating classical pro-inflammatory monocytes and increase of alternative M2 macrophage subtypes in the spleen and CNS.
Interpretation: Our results suggest an anti-inflammatory property of ketamine that can skew macrophages to an M2-like phenotype, highlighting potential therapeutic implications not only for patients with MDD but also other inflammatory-based diseases.
Funding: This study was supported by grants from the Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET) and Agencia Nacional de Promoción Científica y Tecnológica (ANPCyT-FONCYT).
Keywords: Anti-inflammatory M2 macrophages; Depression; IL-12; Ketamine; NMDAR; Non-classical monocytes; mTOR pathway.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors have declared no potential conflicts of interest
Figures






References
-
- Marcus M, Yasamy M, van Ommeren M, Chisholm D, Saxena S. Depression: a global public health concern. [Internet]. 2012 [cited 2016 Agost 25th].
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
