

Immune Reconstitution Inflammatory Syndrome in children
- PMID: 31754484
- PMCID: PMC6837832
- DOI: 10.4102/sajr.v21i2.1257
Immune Reconstitution Inflammatory Syndrome in children
Abstract
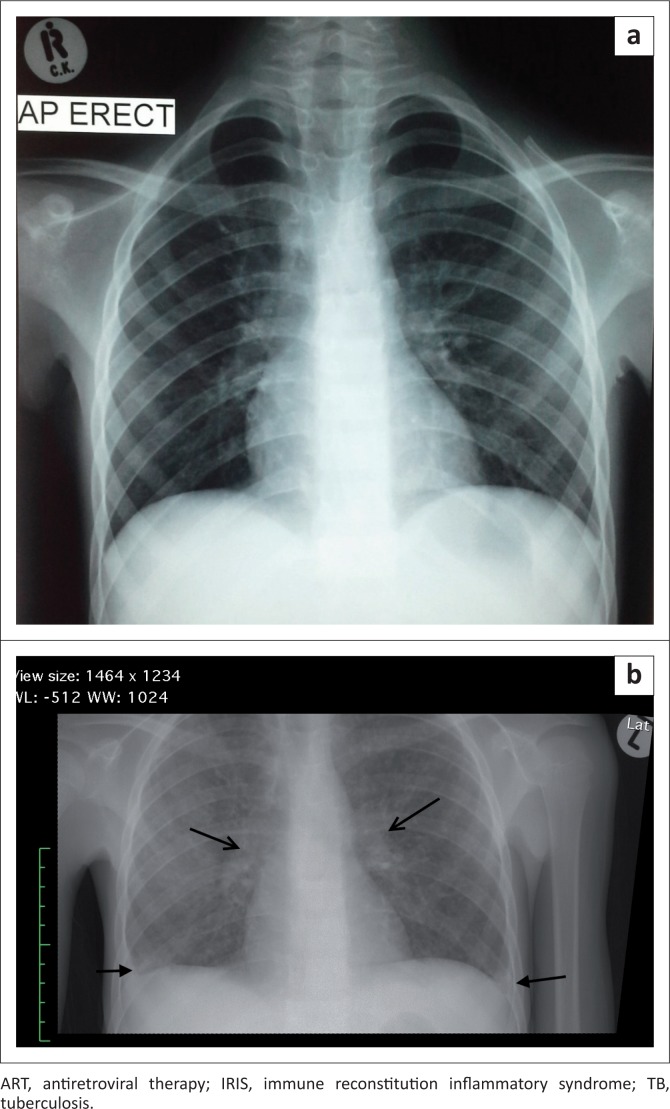
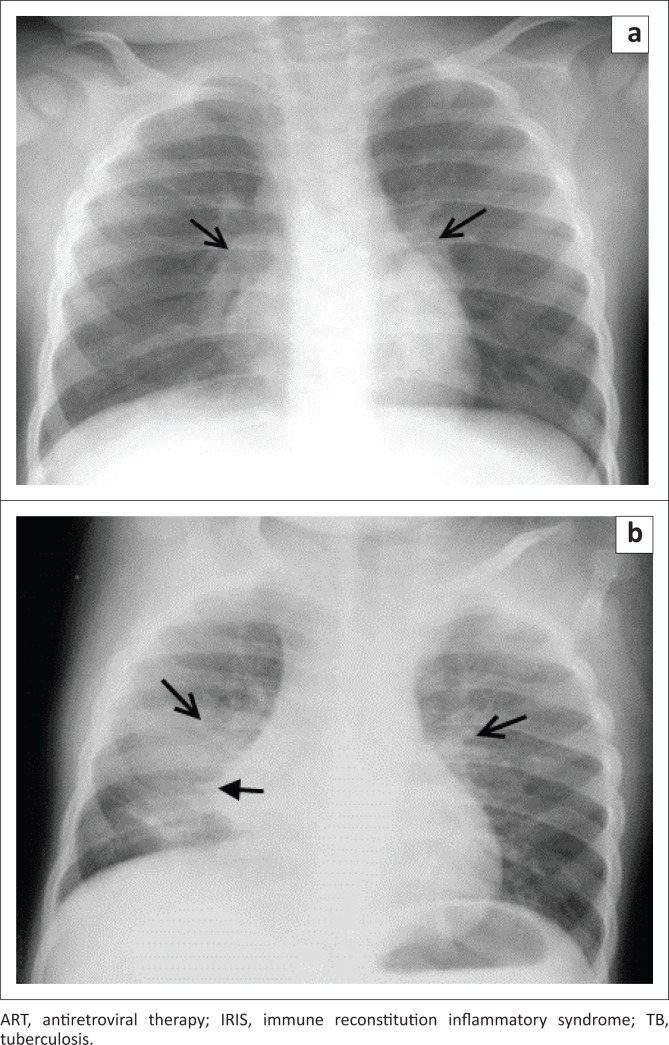
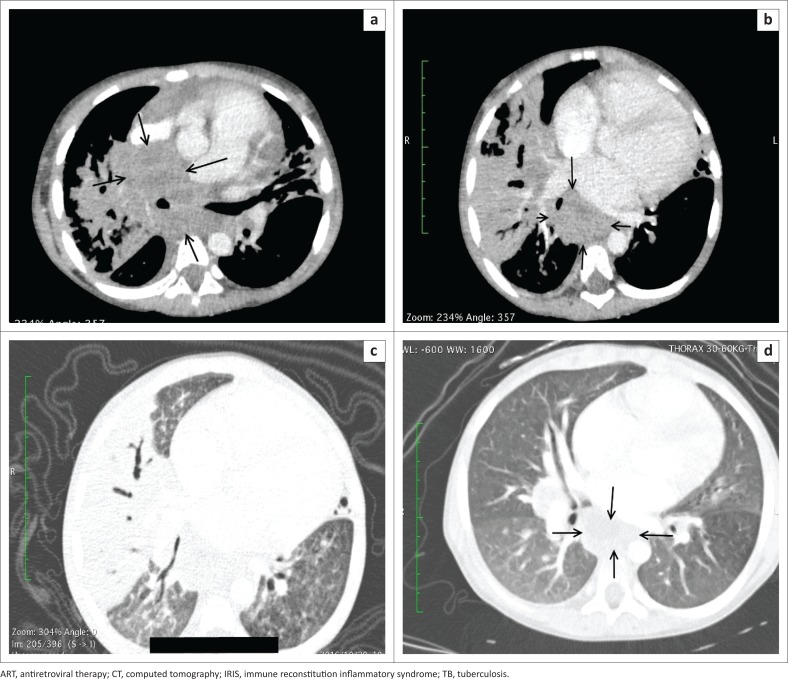
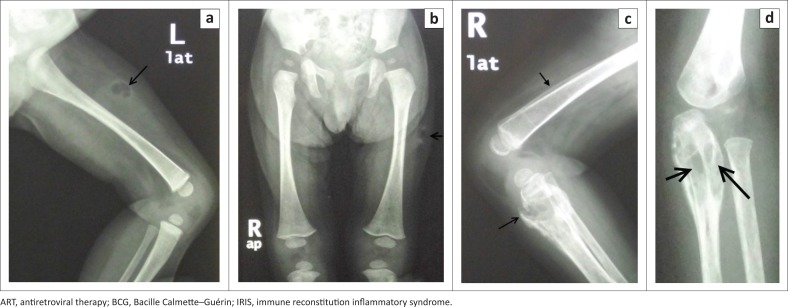
Immune Reconstitution Inflammatory Syndrome (IRIS) refers to a collection of inflammatory disorders, predominantly related to infectious processes that manifest after the initiation of antiretroviral therapy (ART) and can be classified as unmasking or paradoxical. The prevalence of IRIS in children in sub-Saharan Africa is low. Approximately half of all cases are associated with Mycobacterium tuberculosis. It may be difficult to distinguish IRIS from tuberculosis and other opportunistic infections radiologically; therefore, radiological findings must be interpreted with clinical and laboratory findings. In this review article, we describe the clinical and radiological manifestations of IRIS in children and provide illustrative radiological examples.
© 2017. The Authors.
Conflict of interest statement
The authors declare that they have no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
Figures
References
-
- Nesheim SR, Kapogiannis BG, Soe MM, et al. Trends in opportunistic infections in the pre- and post-highly active antiretroviral therapy eras among HIV-infected children in the Perinatal AIDS collaborative transmission study, 1986–2004. Pediatrics. 2007;120(1):100–109. 10.1542/peds.2006-2052 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources