

Characterization of Mucosal Dysbiosis of Early Colonic Neoplasia
- PMID: 31754633
- PMCID: PMC6856115
- DOI: 10.1038/s41698-019-0101-6
Characterization of Mucosal Dysbiosis of Early Colonic Neoplasia
Abstract
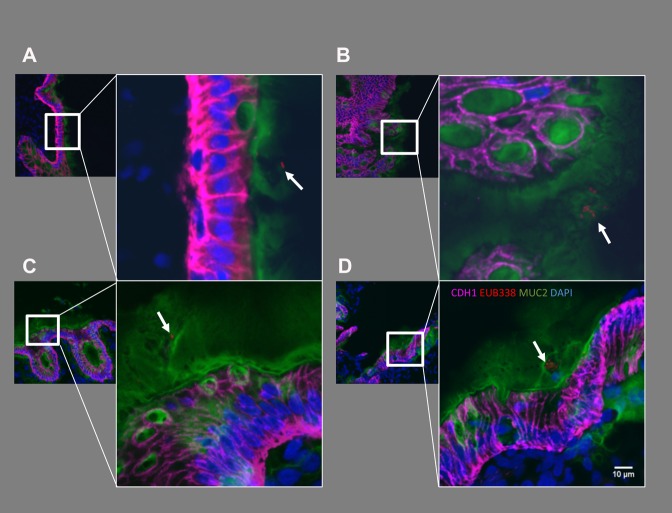
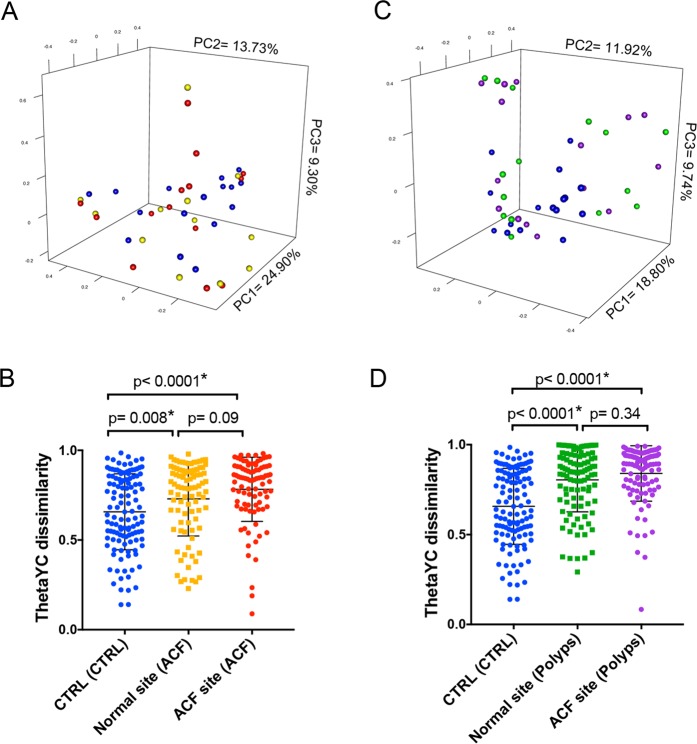
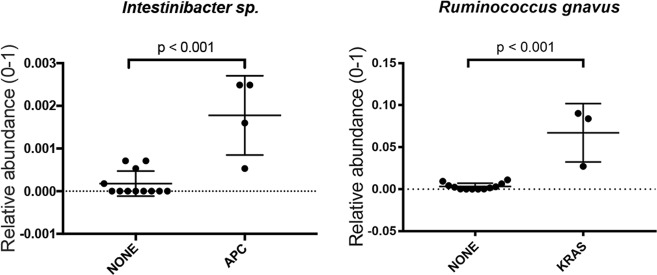
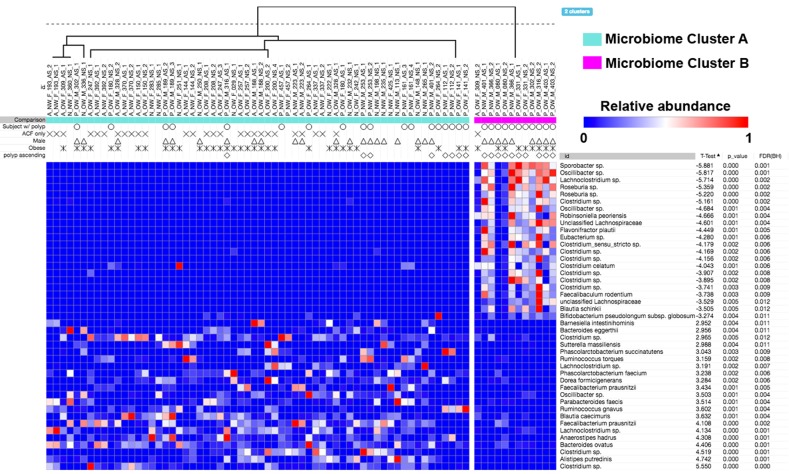
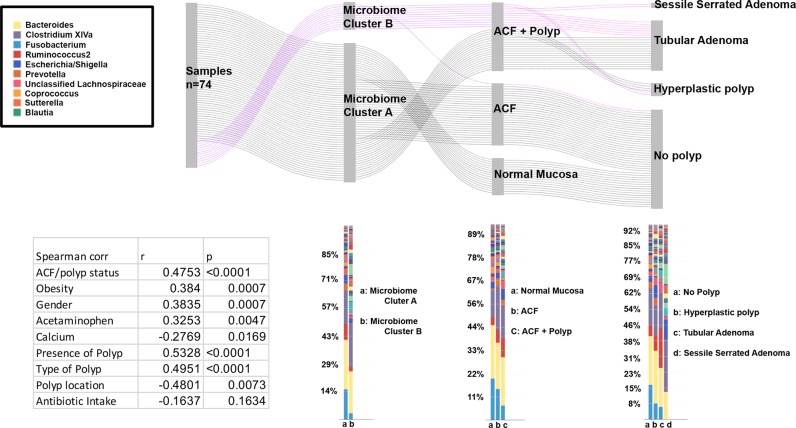
Aberrant crypt foci (ACF) are the earliest morphologically identifiable lesions in the colon that can be detected by high-definition chromoendoscopy with contrast dye spray. Although frequently associated with synchronous adenomas, their role in colorectal tumor development, particularly in the proximal colon, is still not clear. The goal of this study was to evaluate the profile of colon-adherent bacteria associated with proximal ACF and to investigate their relationship to the presence and subtype of synchronous polyps present throughout the colon. Forty-five subjects undergoing a screening or surveillance colonoscopy were included in this retrospective study. Bacterial cells adherent to the epithelia of ACF and normal mucosal biopsies were visualized by in situ hybridization within confocal tissue sections. ACF showed significantly greater heterogeneity in their bacterial microbiome profiles compared with normal mucosa. One of the bacterial community structures we characterized was strongly correlated with the presence of synchronous polyps. Finally, using DNA mass spectrometry to evaluate a panel of colorectal cancer hotspot mutations present in the ACF, we found that three APC gene mutations were positively associated with the presence of Instestinibacter sp., whereas KRAS mutations were positively correlated with Ruminococcus gnavus. This result indicates a potential relationship between specific colon-associated bacterial species and somatically acquired CRC-related mutations. Overall, our findings suggest that perturbations to the normal adherent mucosal flora may constitute a risk factor for early neoplasia, demonstrating the potential impact of mucosal dysbiosis on the tissue microenvironment and behavior of ACF that may facilitate their progression towards more advanced forms of neoplasia.
Keywords: Cancer prevention; Predictive markers.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
