

Clinical and genetic correlates of islet-autoimmune signatures in juvenile-onset type 1 diabetes
- PMID: 31754749
- PMCID: PMC6946733
- DOI: 10.1007/s00125-019-05032-3
Clinical and genetic correlates of islet-autoimmune signatures in juvenile-onset type 1 diabetes
Abstract
Aims/hypothesis: Heterogeneity in individuals with type 1 diabetes has become more generally appreciated, but has not yet been extensively and systematically characterised. Here, we aimed to characterise type 1 diabetes heterogeneity by creating immunological, genetic and clinical profiles for individuals with juvenile-onset type 1 diabetes in a cross-sectional study.
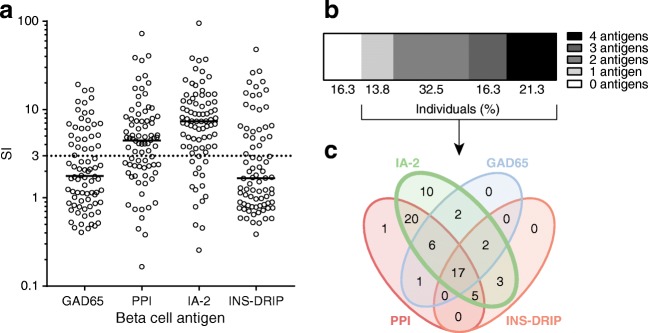
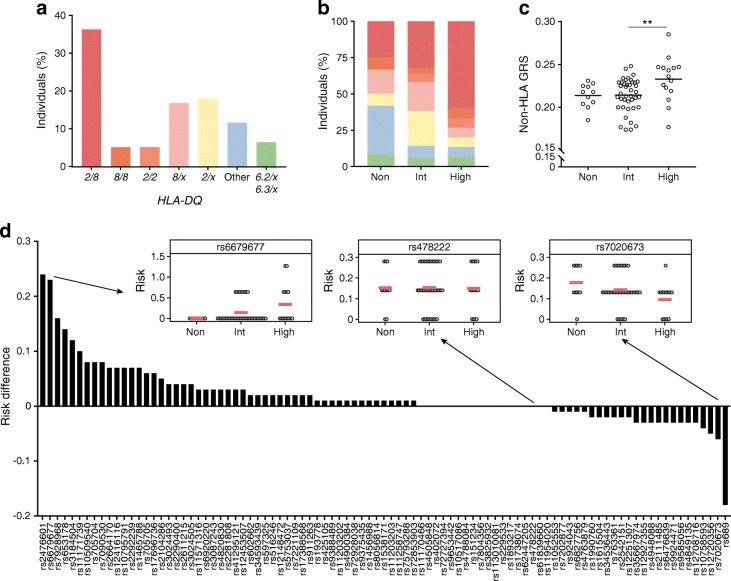
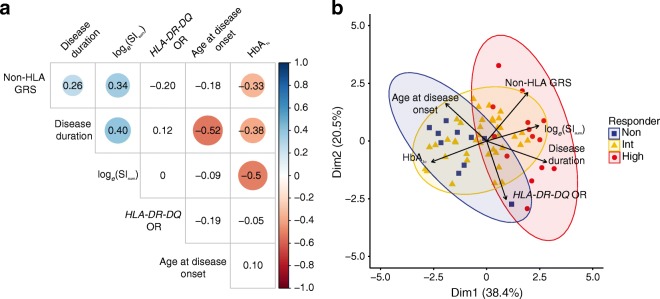
Methods: Participants were HLA-genotyped to determine HLA-DR-DQ risk, and SNP-genotyped to generate a non-HLA genetic risk score (GRS) based on 93 type 1 diabetes-associated SNP variants outside the MHC region. Islet autoimmunity was assessed as T cell proliferation upon stimulation with the beta cell antigens GAD65, islet antigen-2 (IA-2), preproinsulin (PPI) and defective ribosomal product of the insulin gene (INS-DRIP). Clinical parameters were collected retrospectively.
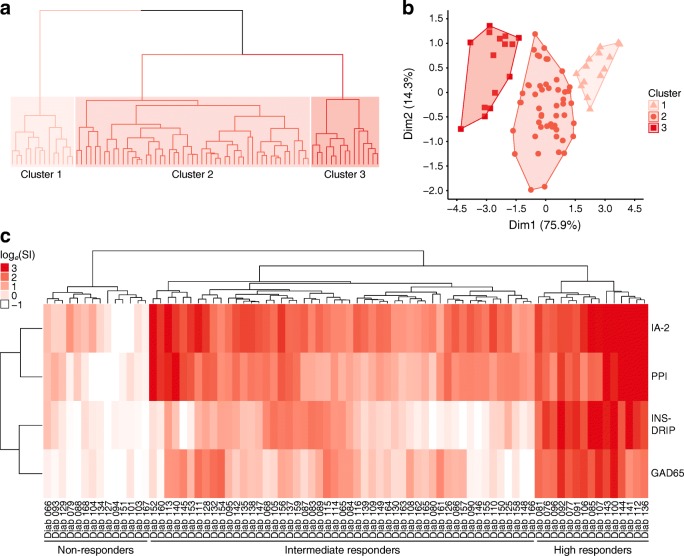
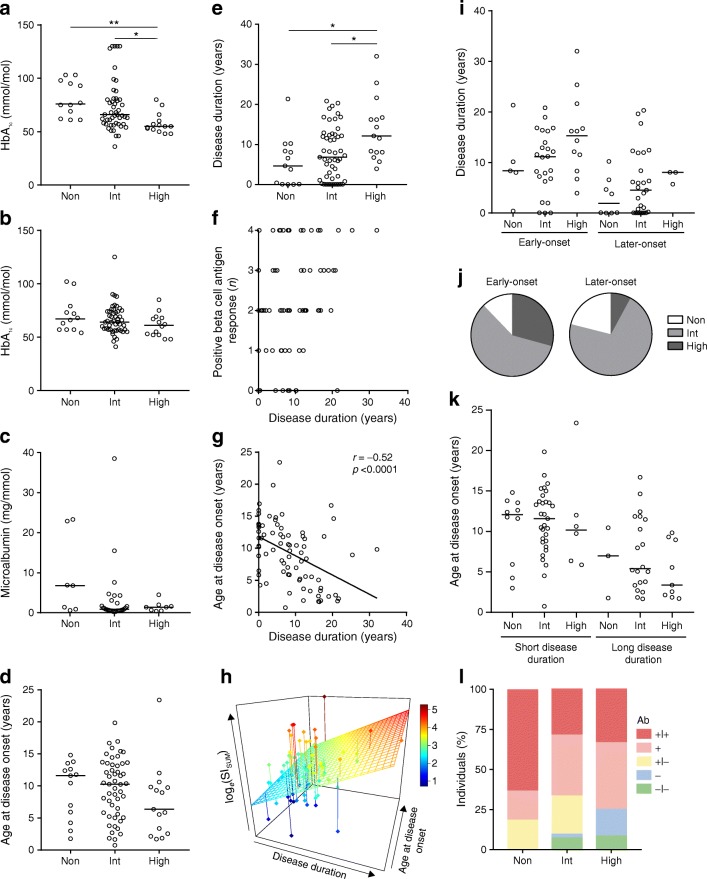
Results: Of 80 individuals, 67 had proliferation responses to one or more islet antigens, with vast differences in the extent of proliferation. Based on the multitude and amplitude of the proliferation responses, individuals were clustered into non-, intermediate and high responders. High responders could not be characterised entirely by enrichment for the highest risk HLA-DR3-DQ2/DR4-DQ8 genotype. However, high responders did have a significantly higher non-HLA GRS. Clinically, high T cell responses to beta cell antigens did not reflect in worsened glycaemic control, increased complications, development of associated autoimmunity or younger age at disease onset. The number of beta cell antigens that an individual responded to increased with disease duration, pointing to chronic islet autoimmunity and epitope spreading.
Conclusions/interpretation: Collectively, these data provide new insights into type 1 diabetes disease heterogeneity and highlight the importance of stratifying patients on the basis of their genetic and autoimmune signatures for immunotherapy and personalised disease management.
Keywords: Autoimmune disease; Autoreactive T cells; Disease endotypes; Disease heterogeneity; Epitope spreading; Immunotherapy; Islet autoantigen; Patient heterogeneity; Personalised medicine; Precision medicine.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
