

Robot assisted versus laparoscopic suturing learning curve in a simulated setting
- PMID: 31754849
- PMCID: PMC7326898
- DOI: 10.1007/s00464-019-07263-2
Robot assisted versus laparoscopic suturing learning curve in a simulated setting
Abstract
Background: Compared to conventional laparoscopy, robot assisted surgery is expected to have most potential in difficult areas and demanding technical skills like minimally invasive suturing. This study was performed to identify the differences in the learning curves of laparoscopic versus robot assisted suturing.
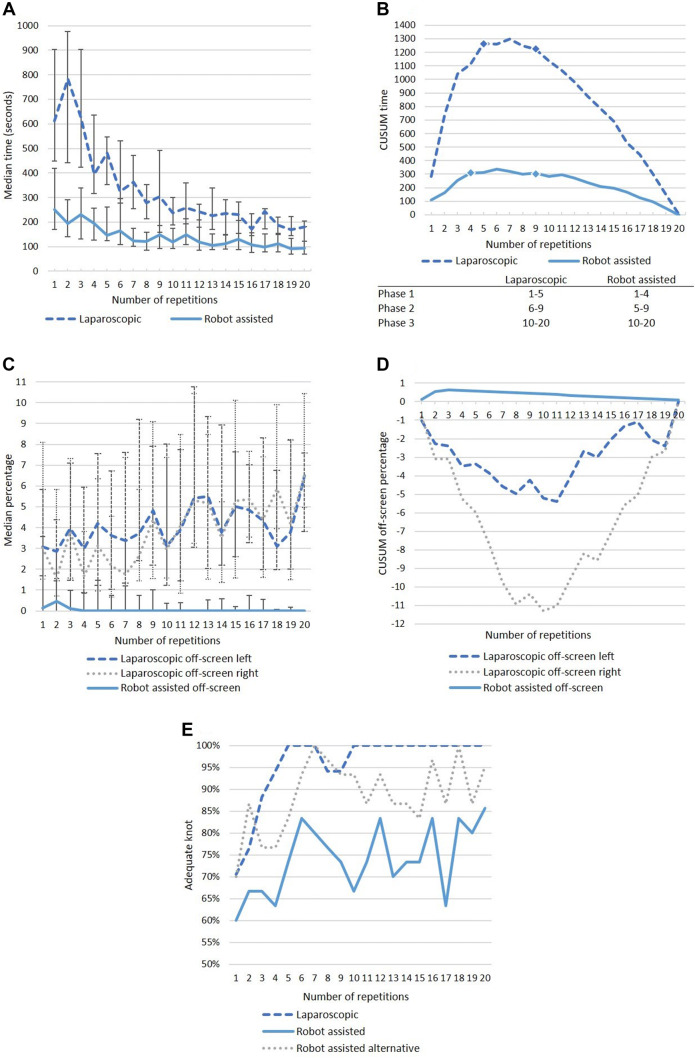
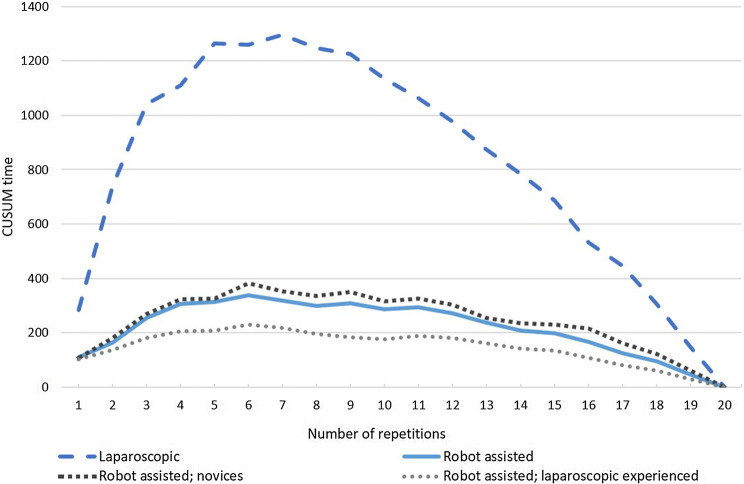
Method: Novice participants performed three suturing tasks on the EoSim laparoscopic augmented reality simulator or the RobotiX robot assisted virtual reality simulator. Each participant performed an intracorporeal suturing task, a tilted plane needle transfer task and an anastomosis needle transfer task. To complete the learning curve, all tasks were repeated up to twenty repetitions or until a time plateau was reached. Clinically relevant and comparable parameters regarding time, movements and safety were recorded. Intracorporeal suturing time and cumulative sum analysis was used to compare the learning curves and phases.
Results: Seventeen participants completed the learning curve laparoscopically and 30 robot assisted. Median first knot suturing time was 611 s (s) for laparoscopic versus 251 s for robot assisted (p < 0.001), and this was 324 s versus 165 (sixth knot, p < 0.001) and 257 s and 149 s (eleventh knot, p < 0.001) respectively on base of the found learning phases. The percentage of 'adequate surgical knots' was higher in the laparoscopic than in the robot assisted group. First knot: 71% versus 60%, sixth knot: 100% versus 83%, and eleventh knot: 100% versus 73%. When assessing the 'instrument out of view' parameter, the robot assisted group scored a median of 0% after repetition four. In the laparoscopic group, the instrument out of view increased from 3.1 to 3.9% (left) and from 3.0 to 4.1% (right) between the first and eleventh knot (p > 0.05).
Conclusion: The learning curve of minimally invasive suturing shows a shorter task time curve using robotic assistance compared to the laparoscopic curve. However, laparoscopic outcomes show good end results with rapid outcome improvement.
Keywords: Laparoscopy training; Learning curve; Robotics training; Simulation.
Conflict of interest statement
Erik Leijte, Ivo De Blaauw, Frans Van Workum, Camiel Rosman, and Sanne Botden have no conflicts of interest or financial ties to disclose.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
