

Constrained Optimization for the Selection of Influenza Vaccines to Maximize the Population Benefit: A Demonstration Project
- PMID: 31755016
- PMCID: PMC7347519
- DOI: 10.1007/s40258-019-00534-y
Constrained Optimization for the Selection of Influenza Vaccines to Maximize the Population Benefit: A Demonstration Project
Abstract
Background: Influenza is an infectious disease causing a high annual economic and public health burden. The most efficient management of the disease is through prevention with vaccination. Many influenza vaccines are available, with varying efficacy and cost, targeting different age groups. Therefore, strategic decision-making about which vaccine to deliver to whom is warranted to improve efficiency.
Objective: We present the use of a constrained optimization (CO) model to evaluate targeted strategies for providing influenza vaccines in three adult age groups in the USA.
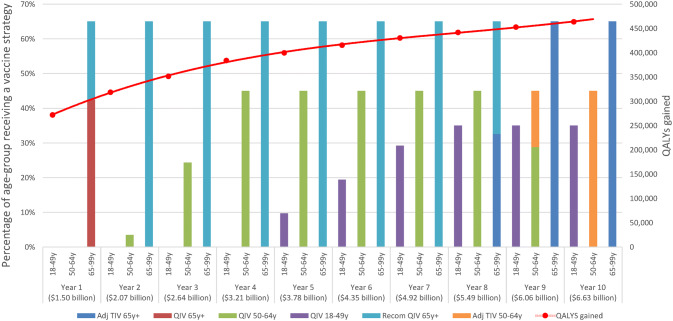
Methods: CO was considered for identifying an influenza vaccine provision strategy that maximizes the benefits at constrained annual budgets, by prioritizing vaccines based on return on investment. The approach optimizes a set of predefined outcome measures over several years resulting from an increasing investment using the best combination of influenza vaccines.
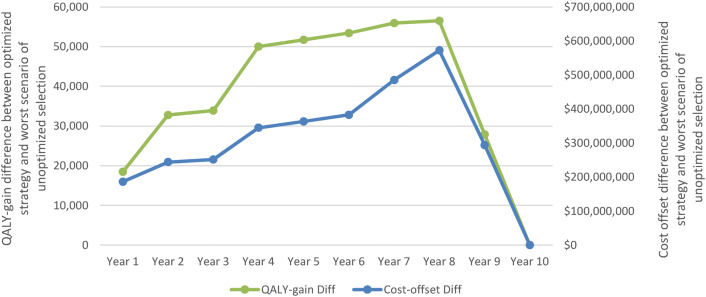
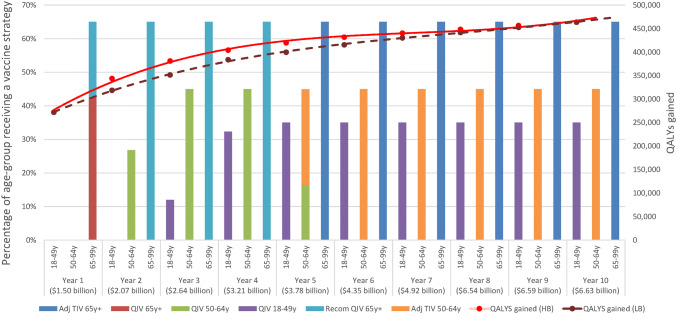
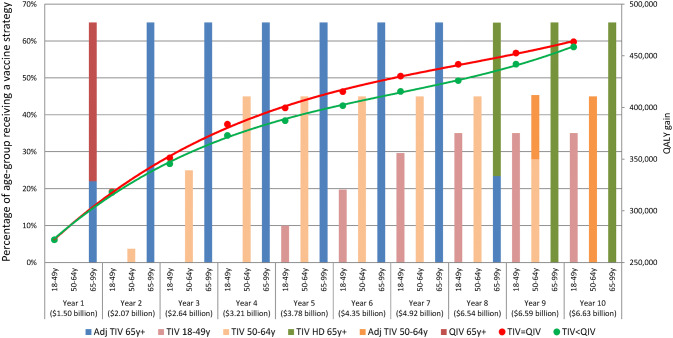
Results: Results indicate the importance of understanding the relative differences in benefits for each vaccine type within and across age groups. Scenario and threshold analyses demonstrate the impact of changing budget distribution over time, price setting per vaccine type, and selection of outcome measure to optimize.
Conclusion: Significant gains in cost efficiency can be realized for a decision maker using a CO model, especially for a disease like influenza with many vaccine options. Testing the model under different scenarios offers powerful insights into maximum achievable benefit overall and per age group within the predefined constraints of a vaccine budget.
Conflict of interest statement
B. Standaert and P. Buck are employees of the GSK group of companies and declare restricted shares ownership in the GSK group of companies. I. Van Vlaenderen, L.A. Van Bellinghen, S. Talbird, K. Hicks, and J. Carrico declare that their institutions have received fees from the GSK group of companies during the conduct of the study reported here as well as for projects outside the submitted work.
Figures
Comment in
-
The Potential Role of Constrained Optimization Methods in Healthcare Decision Making.Appl Health Econ Health Policy. 2020 Aug;18(4):461-462. doi: 10.1007/s40258-020-00559-8. Appl Health Econ Health Policy. 2020. PMID: 32034670 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
