

The Demographics of Fractures and Dislocations Across the Entire United States due to Common Sports and Recreational Activities
- PMID: 31755815
- PMCID: PMC7040946
- DOI: 10.1177/1941738119882930
The Demographics of Fractures and Dislocations Across the Entire United States due to Common Sports and Recreational Activities
Abstract
Background: There exists little nationwide data regarding fracture and dislocation patterns across a wide variety of sporting activities for all ages and sexes.
Hypothesis: Participant demographics (age and sex) will vary with regard to fracture and joint dislocation sustained during sport-related activities.
Study design: Descriptive epidemiology study.
Level of evidence: Level 3.
Methods: The National Electronic Injury Surveillance System All Injury Program data 2005 through 2013 were accessed; 18 common sports and recreational activities in the United States were selected. Statistical software was used to calculate the numbers of fractures and dislocations, and incidence was calculated using US Census Bureau data. Multivariate logistic regression analysis determined the odds ratios (ORs) for the occurrence of a fracture or dislocation.
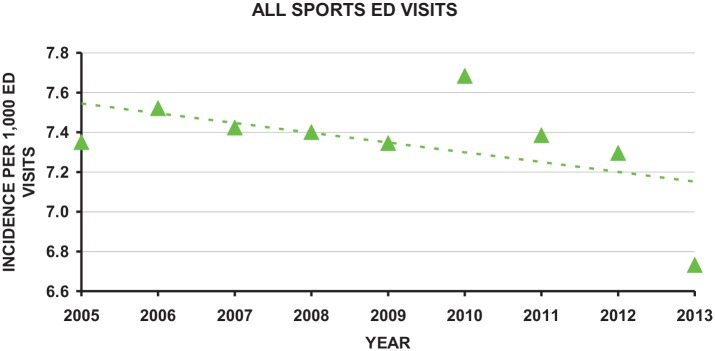
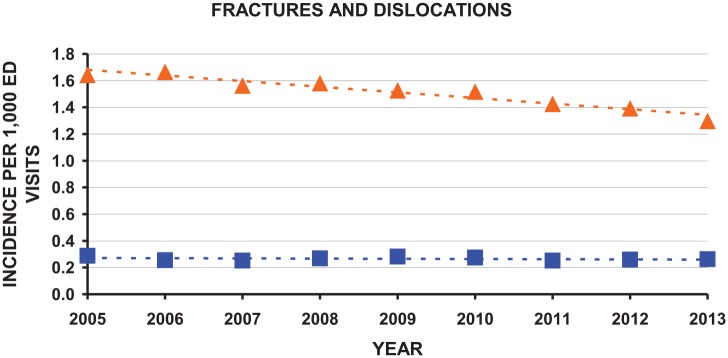
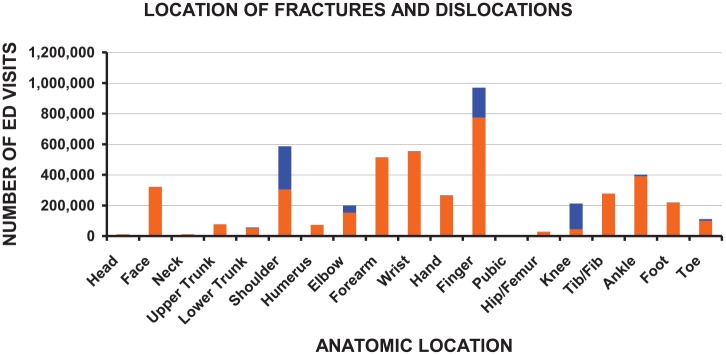
Results: A fracture occurred in 20.6% and a joint dislocation in 3.6% of the emergency department visits for sports-related injuries; annual emergency department visit incidence was 1.51 for fractures and 0.27 for dislocations (per 1000 people). Most of the fractures occurred in football (22.5%). The OR for fracture was highest for inline skating (OR, 6.03), males (OR, 1.21), Asians, whites, and Amerindians compared with blacks (OR, 1.46, 1.25, and 1.18, respectively), and those older than 84 years (OR, 4.77). Most of the dislocations occurred in basketball (25.7%). The OR for dislocation was highest in gymnastics (OR, 4.08), males (OR, 1.50), Asians (OR, 1.75), and in those aged 20 to 24 years (OR, 9.04). The most common fracture involved the finger, and the most common dislocation involved the shoulder.
Conclusion: Inline skating had the greatest risk for fracture, and gymnastics had the greatest risk for joint dislocation.
Clinical relevance: This comprehensive study of the risks of sustaining a fracture or dislocation from common sports activities across all age groups can aid sports health providers in a better understanding of those sports at high risk and be proactive in prevention mechanisms (protective gear, body training).
Keywords: NEISS; demographic; dislocation; fracture; recreation; sport.
Conflict of interest statement
The authors report no potential conflicts of interest in the development and publication of this article.
Figures
References
-
- Annest JL, Mercy JA, Gibson DR, Ryan GW. National estimates of nonfatal firearm-related injuries. Beyond the tip of the iceberg. JAMA. 1995;273:1749-1754. - PubMed
-
- Atkin DM, Fithian DC, Marangi KS, Stone ML, Dobson BE, Mendelsohn C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med. 2000;28:472-479. - PubMed
-
- Aydin A, Atmaca H, Müezzinoğlu ÜS. Anterior knee dislocation with ipsilateral open tibial shaft fracture: a 5-year clinical follow-up of a professional athlete. Musculoskelet Surg. 2013;97:165-168. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
