

Cognitive Behavioral Treatments for Anxiety in Children With Autism Spectrum Disorder: A Randomized Clinical Trial
- PMID: 31755906
- PMCID: PMC6902190
- DOI: 10.1001/jamapsychiatry.2019.4160
Cognitive Behavioral Treatments for Anxiety in Children With Autism Spectrum Disorder: A Randomized Clinical Trial
Abstract
Importance: Anxiety is common among youth with autism spectrum disorder (ASD), often interfering with adaptive functioning. Psychological therapies are commonly used to treat school-aged youth with ASD; their efficacy has not been established.
Objective: To compare the relative efficacy of 2 cognitive behavioral therapy (CBT) programs and treatment as usual (TAU) to assess treatment outcomes on maladaptive and interfering anxiety in children with ASD. The secondary objectives were to assess treatment outcomes on positive response, ASD symptom severity, and anxiety-associated adaptive functioning.
Design, setting, and participants: This randomized clinical trial began recruitment in April 2014 at 3 universities in US cities. A volunteer sample of children (7-13 years) with ASD and maladaptive and interfering anxiety was randomized to standard-of-practice CBT, CBT adapted for ASD, or TAU. Independent evaluators were blinded to groupings. Data were collected through January 2017 and analyzed from December 2018 to February 2019.
Interventions: The main features of standard-of-practice CBT were affect recognition, reappraisal, modeling/rehearsal, in vivo exposure tasks, and reinforcement. The CBT intervention adapted for ASD was similar but also addressed social communication and self-regulation challenges with perspective-taking training and behavior-analytic techniques.
Main outcomes and measures: The primary outcome measure per a priori hypotheses was the Pediatric Anxiety Rating Scale. Secondary outcomes included treatment response on the Clinical Global Impressions-Improvement scale and checklist measures.
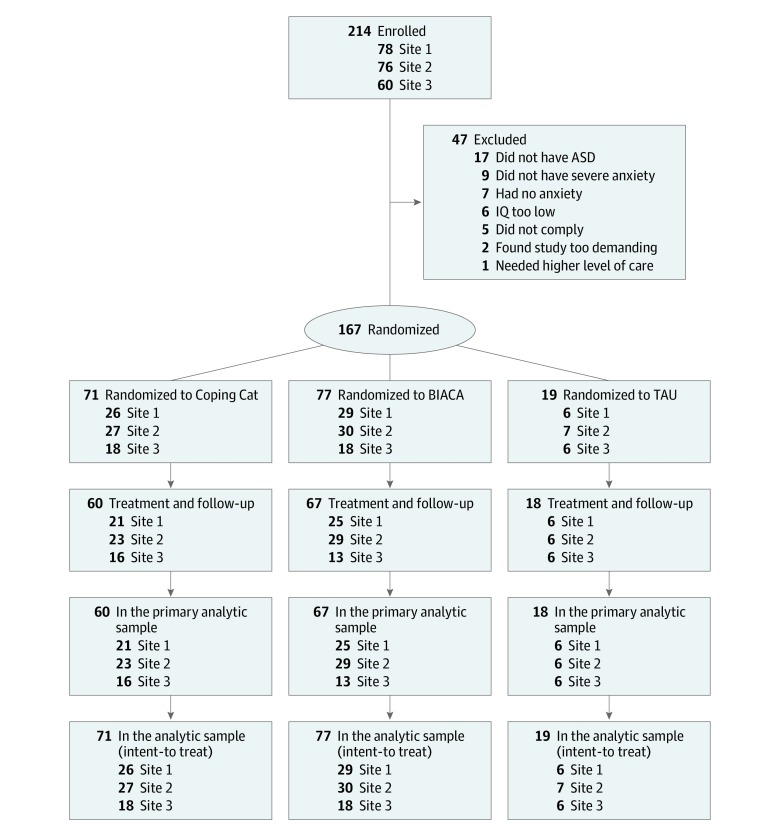
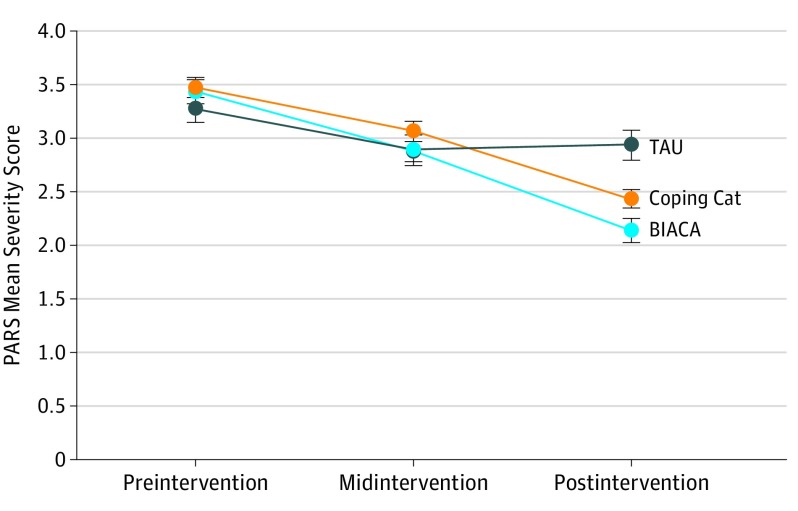
Results: Of 214 children initially enrolled, 167 were randomized, 145 completed treatment, and 22 discontinued participation. Those who were not randomized failed to meet eligibility criteria (eg, confirmed ASD). There was no significant difference in discontinuation rates across conditions. Randomized children had a mean (SD) age of 9.9 (1.8) years; 34 were female (20.5%). The CBT program adapted for ASD outperformed standard-of-practice CBT (mean [SD] Pediatric Anxiety Rating Scale score, 2.13 [0.91] [95% CI, 1.91-2.36] vs 2.43 [0.70] [95% CI, 2.25-2.62]; P = .04) and TAU (2.93 [0.59] [95% CI, 2.63-3.22]; P < .001). The CBT adapted for ASD also outperformed standard-of-practice CBT and TAU on parent-reported scales of internalizing symptoms (estimated group mean differences: adapted vs standard-of-practice CBT, -0.097 [95% CI, -0.172 to -0.023], P = .01; adapted CBT vs TAU, -0.126 [95% CI, -0.243 to -0.010]; P = .04), ASD-associated social-communication symptoms (estimated group mean difference: adapted vs standard-of-practice CBT, -0.115 [95% CI, -0223 to -0.007]; P = .04; adapted CBT vs TAU: -0.235 [95% CI,-0.406 to -0.065]; P = .01); and anxiety-associated social functioning (estimated group mean difference: adapted vs standard-of-practice CBT, -0.160 [95% CI, -0.307 to -0.013]; P = .04; adapted CBT vs TAU: -0.284 [95% CI, -0.515 to -0.053]; P = .02). Both CBT conditions achieved higher rates of positive treatment response than TAU (BIACA, 61 of 66 [92.4%]; Coping Cat, 47 of 58 [81.0%]; TAU, 2 of 18 [11.1%]; P < .001 for each comparison).
Conclusions and relevance: In this study, CBT was efficacious for children with ASD and interfering anxiety, and an adapted CBT approach showed additional advantages. It is recommended that clinicians providing psychological treatments to school-aged children with ASD consider developing CBT expertise.
Trial registration: ClinicalTrials.gov identifier: NCT02028247.
Conflict of interest statement
Figures
References
-
- White SW, Mazefsky CA, Dichter GS, Chiu PH, Richey JA, Ollendick TH. Social-cognitive, physiological, and neural mechanisms underlying emotion regulation impairments: understanding anxiety in autism spectrum disorder. Int J Dev Neurosci. 2014;39:22-36. doi: 10.1016/j.ijdevneu.2014.05.012 - DOI - PMC - PubMed
-
- Kerns CM, Kendall PC. The presentation and classification of anxiety in autism spectrum disorder. Clin Psychol. 2012;19(4):323-347. doi: 10.1111/cpsp.12009 - DOI
