

Liver transplantation in propionic and methylmalonic acidemia: A single center study with literature review
- PMID: 31757659
- PMCID: PMC6898966
- DOI: 10.1016/j.ymgme.2019.11.001
Liver transplantation in propionic and methylmalonic acidemia: A single center study with literature review
Abstract
Background: Organic acidemias, especially propionic acidemia (PA) and methylmalonic acidemia (MMA), may manifest clinically within the first few hours to days of life. The classic presentation in the newborn period includes metabolic acidosis, hyperlactatemia, and hyperammonemia that is precipitated by unrestricted protein intake. Implementation of newborn screening to diagnose and initiate early treatment has facilitated a reduction in neonatal mortality and improved survival. Despite early diagnosis and appropriate management, these individuals are prone to have recurrent episodes of metabolic acidosis and hyperammonemia resulting in frequent hospitalizations. Liver transplantation (LT) has been proposed as a treatment modality to reduce metabolic decompensations which are not controlled by medical management. Published reports on the outcome of LT show heterogeneous results regarding clinical and biochemical features in the post transplantation period. As a result, we evaluated the outcomes of LT in our institution and compared it to the previously published data.
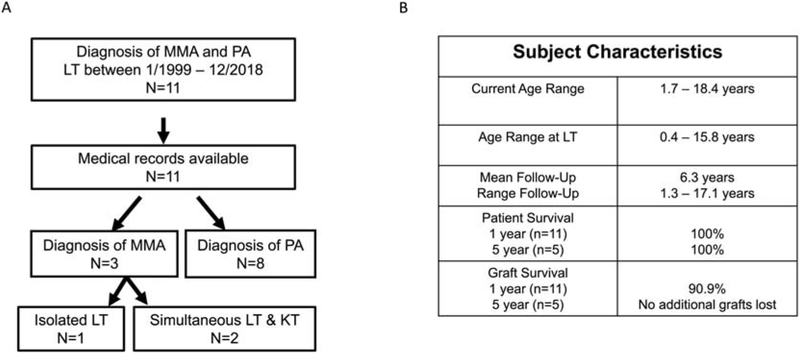
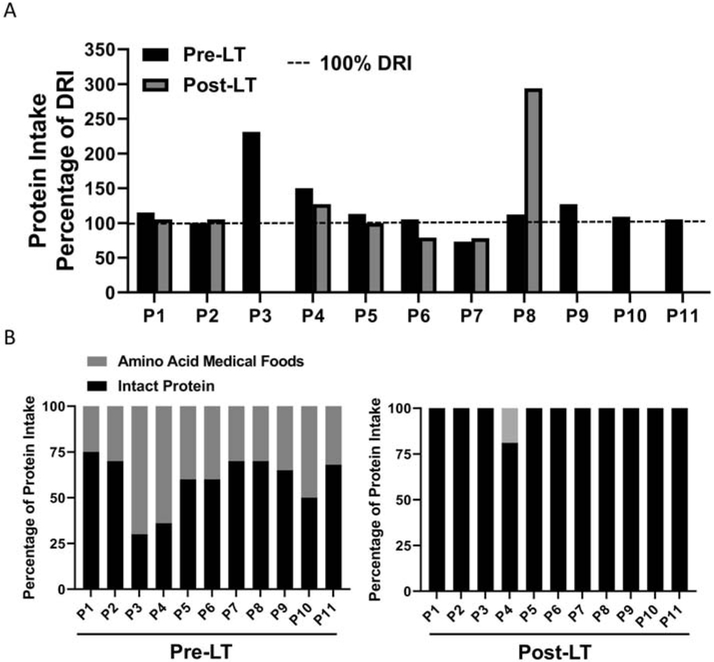
Study design/methods: We performed a retrospective chart review of nine individuals with PA or MMA who underwent LT and two individuals with MMA who underwent LT and kidney transplantation (KT). Data including number of hospitalizations, laboratory measures, cardiac and neurological outcomes, dietary protein intake, and growth parameters were collected.
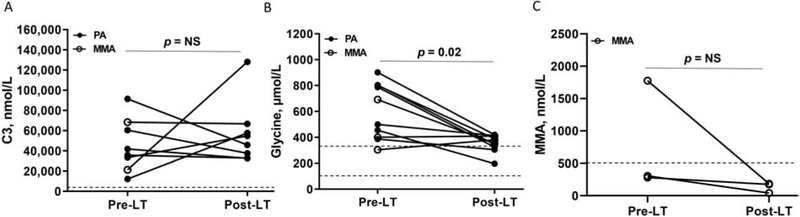
Results: The median age of transplantation for subjects with MMA was 7.2 years with a median follow up of 4.3 years. The median age of transplantation for subjects with PA was 1.9 years with a median follow up of 5.4 years. The survival rate at 1 year and 5 years post-LT was 100%. Most of our subjects did not have any episodes of hyperammonemia or pancreatitis post-LT. There was significant reduction in plasma glycine post-LT. One subject developed mild elevation in ammonia post-LT on an unrestricted protein diet, suggesting that protein restriction may be indicated even after LT.
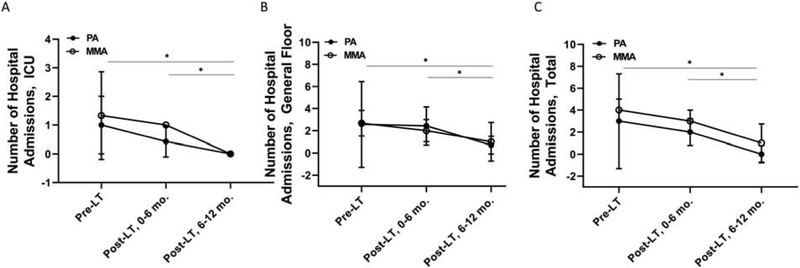
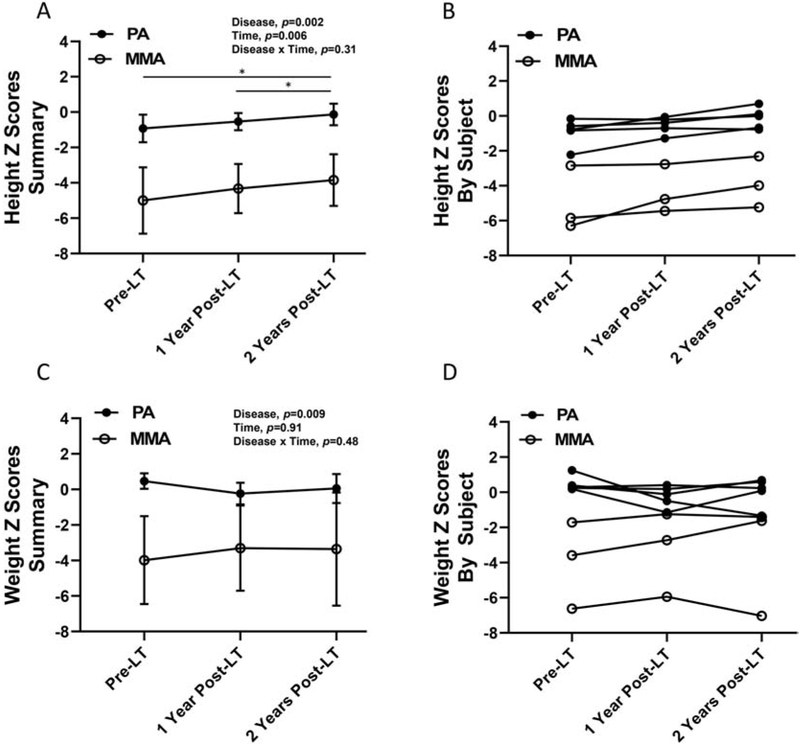
Conclusion: In a large single center study of LT in MMA and PA, we show that LT may reduce the incidence of metabolic decompensation. Moreover, our data suggest that LT may be associated with reduced number of hospitalizations and improved linear growth in individuals with PA and MMA.
Keywords: Liver transplantation; Methylmalonic acidemia; Organic acidemia; Propionic acidemia.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: None
Figures
References
-
- Chace DH, DiPerna JC, Kalas TA, Johnson RW, Naylor EW, Rapid diagnosis of methylmalonic and propionic acidemias: Quantitative tandem mass spectrometric analysis of propionylcarnitine in filter-paper blood specimens obtained from newborns, Clin. Chem 47 (2001) 2040–2044. - PubMed
-
- Couce ML, Castiñeiras DE, Bóveda MD, Baña A, Cocho JA, Iglesias AJ, Colón C, Alonso-Fernández JR, Fraga JM, Evaluation and long-term follow-up of infants with inborn errors of metabolism identified in an expanded screening programme, Mol. Genet. Metab 104 (2011) 470–475. 10.1016/j.ymgme.2011.09.021. - DOI - PubMed
-
- Baumgartner MR, Hörster F, Dionisi-Vici C, Haliloglu G, Karall D, Chapman KA, Huemer M, Hochuli M, Assoun M, Ballhausen D, Burlina A, Fowler B, Grünert SC, Grünewald S, Honzik T, Merinero B, Pérez-Cerdá C, Scholl-Bürgi S, Skovby F, Wijburg F, MacDonald A, Martinelli D, Sass JO, Valayannopoulos V, Chakrapani A, Proposed guidelines for the diagnosis and management of methylmalonic and propionic acidemia, Orphanet J. Rare Dis 9 (2014). 10.1186/s13023-014-0130-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
