

Neuromyelitis optica spectrum disorders with unevenly clustered attack occurrence
- PMID: 31757816
- PMCID: PMC6935841
- DOI: 10.1212/NXI.0000000000000640
Neuromyelitis optica spectrum disorders with unevenly clustered attack occurrence
Abstract
Objective: The aim of this study was to elucidate the characteristics of clinical attacks in neuromyelitis optica spectrum disorders (NMOSDs) with positive serum anti-aquaporin-4 antibody. Both the timing and sequential pattern of clinical types were analyzed.
Methods: A total of 69 patients with NMOSD were enrolled in this study, all of whom were treated at a single university hospital. All data regarding the clinical attacks (including types and date) together with other clinical information were collected.
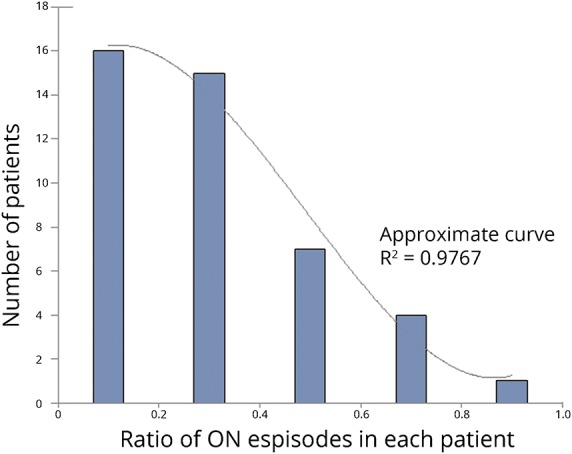
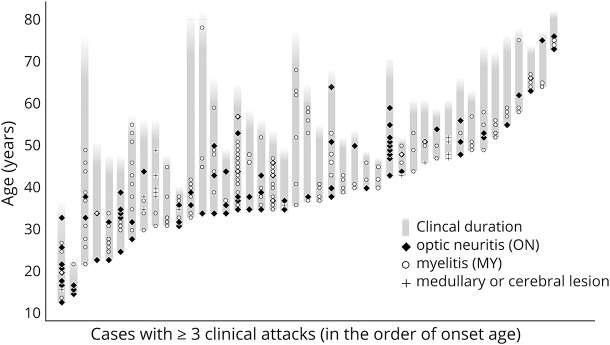
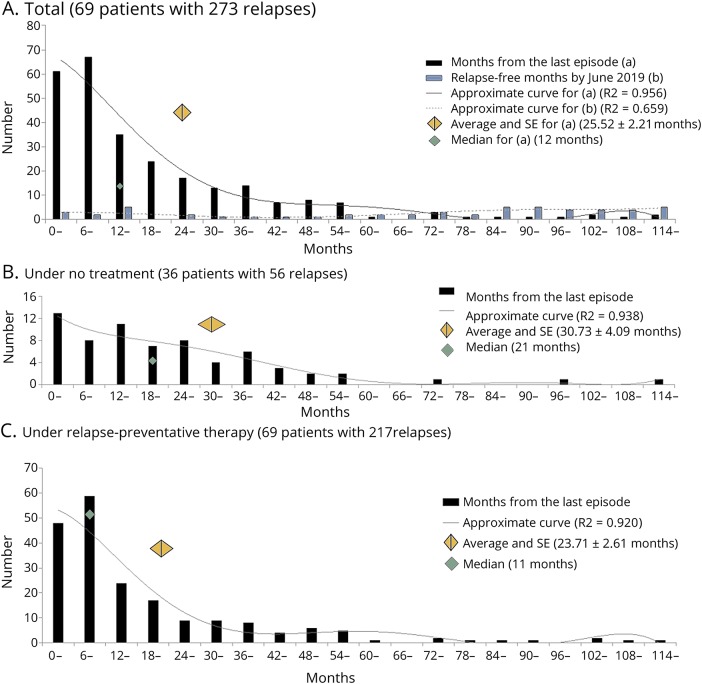
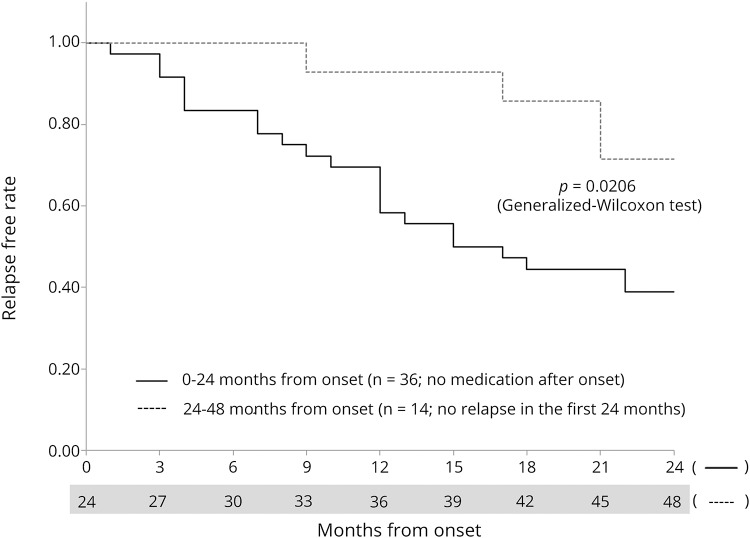
Results: Analysis of clinical attacks from the enrolled patients showed that there were 2 distributional patterns of attack occurrence in each patient: (1) "clustered" occurrences, which occurred within 12 months from the previous attack, and (2) "nonclustered" intermittent occurrences, which occurred ≥12 months after the previous attack. These occurrences were regardless of the duration from the onset. During the "clustered" period, clinical attacks were more likely to show a similar clinical manifestation, such as optic neuritis or myelitis. After entering the "nonclustered" intermittent period, the relapses were of random clinical type, regardless of the previous clinical manifestation.
Conclusions: Patients with NMOSD showed mixed periods of "clustered" occurrence with frequent attacks presenting with similar manifestations and "nonclustered" intermittent periods with sparse relapses. Approximately half of the relapses occurred during the "clustered" period within 12 months of the last clinical attack. Clinicians should pay special attention to whether the patients are presently in the "clustered" or "nonclustered" period to decide optimal relapse-preventive strategies.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources